
Quiz: Are You Ready For The Measles Outbreak?

Ok, after several posts about the Measles “crisis,” let’s see how much you know about the disease and what it’s currently doing to children in the US (2014-15). This little quiz was given on a website designed for physicians and I’ll let you see how well people on the website did on the same questions.
Unimmunized girl in hospital with measles
The Centers for Disease Control and Prevention (CDC) is the organization tasked with controlling diseases in the US so keeps track on all the statistics. As we mentioned, a tourist decided that schlepping a child sick with Measles around a southern California amusement park was better than spending their vacation in their motel room; so, came into contact with thousands of other children waiting in the long lines during the day.
Because the Southern California area is rife with conspiracy theorists refusing to immunize their children, it wasn’t difficult for the virus to settle onto many other children who, being un-immunized, were susceptible – several of whom immediately began to “share the love” by traveling back to their respective homes in distant cities and states.
The investigation wasn’t easy but very conclusive. As the cases began to mount, they were all traceable back to their own trip to that same amusement park on the same date! Those cases also began building their own portfolio of like-minded, un-immunized children AS WELL AS, unfortunately, infants and seriously ill children who could not be immunized themselves.
As of February 6 (2015) 121 cases of the same virus that produced an epidemic in the Philippines last year has inflicted mostly unimmunized children in 17 US states. Here’s the first question, and I’ll make it multiple choice:
QUESTION ONE: A single dose of measles vaccine administered to a child older than 12 months produces protective immunity in what percentage of individuals. 75%, 80%, 90% or 95%?
How effective are immunizations?
If given as scheduled, at 12 months of age, a single immunization against measles gives immunity to 95% of those who received it! It’s highly effective, more so than even what the readers of that medical blog realized – 45% of whom got the correct answer.
An infant under 6 months of age still is receiving a substantial amount of immunity from its mother via shared blood-stream during gestation. Unfortunately, not only do we have a lot of grandmothers who haven’t seen Measles, we now have many mothers with lower immunity levels in their bloodstream than they would have had if they had gotten the full-blown disease themselves.
Having received their immunity from immunizations rather than the full blown disease, the vertical transmission of immunity to their infants is lower than what was documented back when the original guidelines were made. We now know that vaccination at age 6 months appears effective when needed.
The problem arises from the fact that (even if 100% got the shot) the remaining 5% where the immunization didn’t “take” are still enough to keep this very highly virulent virus churning around the country to other un-immunized people!
We’ve got to get the immunity higher than 95% in order to stop the cycles. Once immunity got up to 98% we found the “magic number” and Measles was declared no longer endemic in the US. That simply takes a second shot to catch 95% of those who didn’t get immunity from the first one. If there is a good side to Measles, the virus has NOT seemed to metastasize into something resistant to the immunization… yet! So —
QUESTION TWO: Which of the following is usually the first sign of measles observed by parents or physicians? Sensitivity to light, rash, high fever (>104°F), edema around the eyes or Koplik spots (in the mouth).
Symptoms of Measles
 Most of those taking this test (59%) realized that a high fever was most often the first sign that a child exhibits when they are coming down with Measles. The fever usually lasts for four or more days.
Most of those taking this test (59%) realized that a high fever was most often the first sign that a child exhibits when they are coming down with Measles. The fever usually lasts for four or more days.
The problem is that IF a parent knows their child has been exposed to measles a fever will pretty much mean: “yep, it’s measles!” If, on the other hand, they don’t have such pre-knowledge, a fever can mean a whole lot of things.
The rash doesn’t come till two to four days (or occasionally not at all). Koplik spots often appear the day before the rash but disappear within two days.
Before the fever comes out fully, the child often feels “yukky”: tired, not hungry, red eyes, cough and runny nose.
It’s only through the magnanimity of all those people who listen to medical advice and immunize their children that those who think the entire medical community is out to get them are able to think “cold” or “ear infection” when their unimmunized child gets a fever. This virus is SO MASSIVELY VIRULENT that before the vaccine, any time a child got their first fever their parents feared measles.
Other frequently associated symptoms include photophobia (sensitivity to light), periorbital edema (swelling around the eyes), and myalgias (muscle aches).
QUESTION THREE: Which of the following is NOT a COMMON complication of measles? Otitis Media, Pericarditis, Croup or Sinusitis.
Complication of Measles
This was almost a trick question. All of them are complications, inflammation around the heart (pericarditis) is just not a common one.
The measles virus which most parents take so lightly can crash just about every other organ system in the child’s body. Common infectious complications include: otitis media, interstitial pneumonitis (lung infection), bronchopneumonia (larger airway infection), laryngotracheobronchitis (croup), worsening of Tuberculosis, loss of response to Tb skin tests, encephalomyelitis (brain-nervous system infection), diarrhea, sinusitis, stomatitis (mouth ulcers), subclinical hepatitis (liver failure), lymphadenitis (lymph node infection) and keratitis (leading to blindness).
And those are just the COMMON ones! Less common, fortunately, include hemorrhagic measles (bleeding), purpura fulminans, hepatitis, disseminated intravascular coagulation (unstoppable bleeding everywhere), subacute sclerosing panencephalitis, thrombocytopenia, appendicitis, ileocolitis, pericarditis, myocarditis, acute pancreatitis and hypocalcemia.
Am I getting the point across? Before immunizations EVERY parent knew a child living with the side-effects of having measles. Nearly every neighborhood contained such a child. Most families had lost children to measles and other contagious diseases.
It is a great luxury for parents to live in a world that they can become so complacent about the disease. The immunization actually changed the world. In fact, it completely eradicated one of late-occurring side-effects: subacute sclerosing panencephalitis (SSP). Dealing with SSP was sort of like dealing with SIDS death – it continues to happen but no one knew why.
After measles immunizations were instituted however SSP completely disappeared. That was how we figured out what was causing it in the fist place! SSP was occurring so long (3 or so years) after measles that no one could draw the connection. To this date there has never been a case of SSP in a person who has had the measles shots.
QUESTION FOUR: Which of the following is the quickest method of confirming acute measles? Viral culture, urinalysis, tissue analysis or antibody assay.
Diagnosing/confirming measles
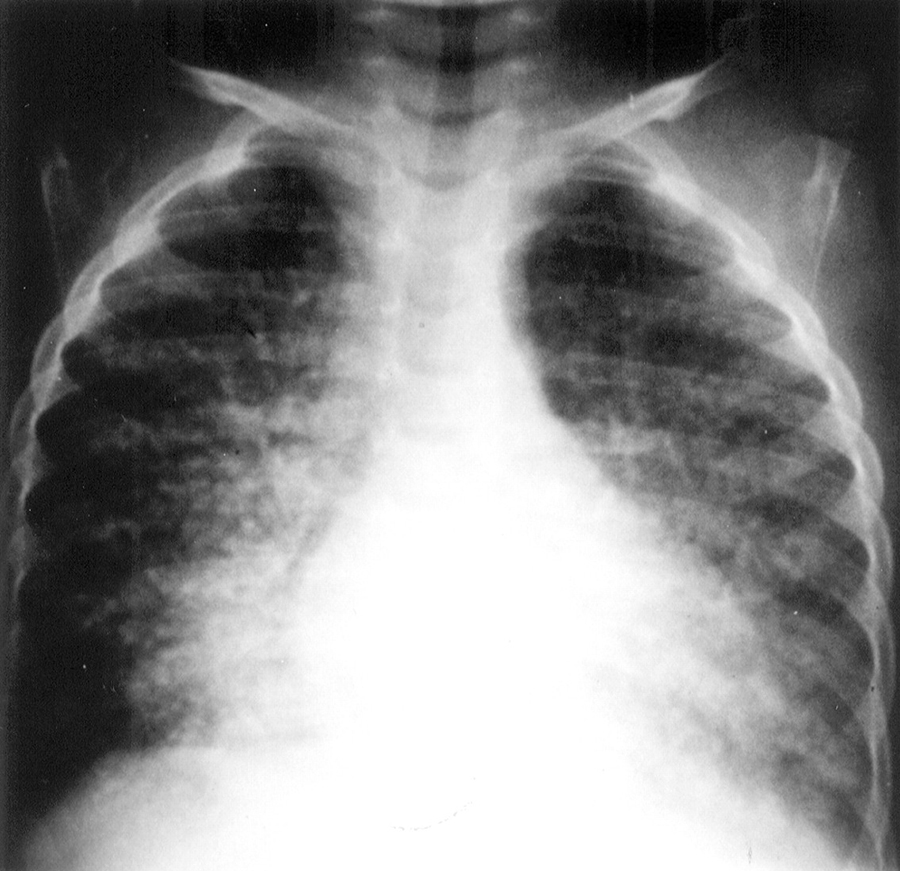 Lung X-ray, Measles Interstitial PneumonitisI didn’t like the way the blog writers wrote this question and thought it was misleading – at least for those of us “codgers” who have actually seen and made the diagnosis many, many times. We sort of fancy that a good patient history and physical exam can make a pretty accurate diagnosis.
Lung X-ray, Measles Interstitial PneumonitisI didn’t like the way the blog writers wrote this question and thought it was misleading – at least for those of us “codgers” who have actually seen and made the diagnosis many, many times. We sort of fancy that a good patient history and physical exam can make a pretty accurate diagnosis.
I guess these days with all the lawyers involved in medicine it should better read the “most legally accurate way.” The “measles virus sandwich-capture immunoglobulin M (IgM) antibody assay,” as it is known, is offered through many local health departments and through the CDC.
I wouldn’t call it the quickest way to “diagnose” because it doesn’t turn positive until after the rash has been visible for at least two days. By then, most of us (as I say) “codgers” would have made the diagnosis and quarantined the child and his contacts.
Perhaps it might be more accurate because there are a whole lot of diseases which cause rashes. And it is a good method when the rash is gone by the time the parent can get the child in, the doc hasn’t ever seen measles personally to know how to diagnose it; or, you need to be 100% accurate for some reason. The test can be run up to a month after the disease.
Now, the last question:
QUESTION FIVE: Which of the following supplementations has been associated with reductions in morbidity and mortality in patients with measles? Calcium, Vitamin D, Vitamin A or Dehydroepiandrosterone (a steroid, sort of)
“Treatment” of measles
Being a virus there is NO antibiotic treatment available. As you should know, no antibiotic anywhere helps any disease caused by any type of virus.
Medicine has developed a couple of medicines which seem to work against some viruses but, unfortunately, there is no medicine available to treat the measles virus once it attacks the body. We have something better! Prevent it entirely with immunization – that wasn’t given as a multiple-choice option though.
Vitamin A was a recent and surprising finding which less than half (44%) of the readers seemed to be aware of.
Vitamin A supplements have been shown to be associated with about 50% reduction in morbidity and mortality from measles and appear to help prevent eye damage and blindness. Not a hundred percent guarantee but we’ll take what we can get!
In fact, if a child is already vitamin A deficient and contracts the measles, the disease is definitely more severe and more likely to develop other significant complications. The World Health Organization (WHO) recommends that all children diagnosed with measles receive vitamin A supplementation, regardless of their country of residence, based on their age.
Did you get that? BASED ON THEIR AGE. That’s because vitamin A is one of the few supplements which can itself cause significant disease (brain) when taken too much!
Vitamin A for treatment of measles
- Vitamin A for treatment of measles is administered once daily for 2 days, at the following doses:
- 200 000 IU for children 12 months or older;
- 100 000 IU for infants 6 through 11 months of age; and
- 50 000 IU for infants younger than 6 months.
- An additional (ie, a third) age-specific dose should be given 2 through 4 weeks later to children with clinical signs and symptoms of vitamin A deficiency.
Both parenteral (IV) and oral formulations of vitamin A are available in the United States. If you’re to the point of using vitamins in measles you really had oughta be talking to your doctor.
[Guidelines for the treatment/prevention of measles. Full text]
Advertisement by Google
(sorry, only few pages have ads)