
“Flu,” “The” Flu or Influenza – Then and Now

Look, there’s a lot screwy about “THE FLU” and enough blame to share about all the confusion. AND, only part of it is about the complete lack of understanding surrounding what to call it.
More•than•once I’ve written posts trying to clarify the name, diagnosis, treatment an how to avoid confusion; but, the issues just seem to feed on themselves and prevent any attempt at understanding.
Influenza virus strikes the youngest and oldest the hardest
Truly, do you understand what is meant when one of your friends claim they have “the Flu?” A hard cold? Vomiting, diarrhea? An earache? Influenza?
They say that this is a “bad flu year”; but, what does that mean?
What The Crud Do You Mean, FLU?
- One—There absolutely is NO medical disease called “stomach flu”! It’s called “gastroenteritis” and there’s no reason to confuse it with a meaningless name
- Two—There are “colds” and there is “Influenza” and they are NOT caused by the same things, even though both are viruses which produce similar symptoms but have vastly different treatments and likely outcomes
- Three—”The Flu” is a non-specific term and basically meaningless except when you’re trying to obtain sympathy for how sick you feel
- Four—There are literally hundreds of different viruses which cause a “cold” and the influenza virus is NOT one of them.
- Five—”Influenza” is a specific disease; caused by a specific virus which has a few different, but similar types; Is controlled/prevented by an immunization; has known and severe complications; and, occurs in epidemics like the one we are currently experiencing.
Influenza: Any Real Advances YET?
The Great Influenza Epidemic of 1918-1919

The current generation (everyone younger than me… and that’s a lot) has absolutely no clue, I’m sure, about the GREAT INFLUENZA of 1918—after all, it was only a footnote at the bottom of the page in their American History text books but we learned about it.
It was, and still is, THE MOST LETHAL INFLUENZA PANDEMIC IN HISTORY and killed between 50 and 100 million people worldwide! It killed more people in a single year than the PLAGUE did in an entire century! There were three distinct “waves” of the illness and death as it spread around the world.
Back then we called it “the Spanish flu”; but, we really don’t know exactly where it started. It may have been amongst the Spanish population in the United States, or not in the Spanish at all.
We had another PANdemic in 2009; but this year, in 2017-18 we are having record-setting hospitalizations and the most severe influenza season in almost a decade.
Is there any difference between THEN and NOW?
Attack and Death Rates
THEN: Pathogenicity and Mortality Rates
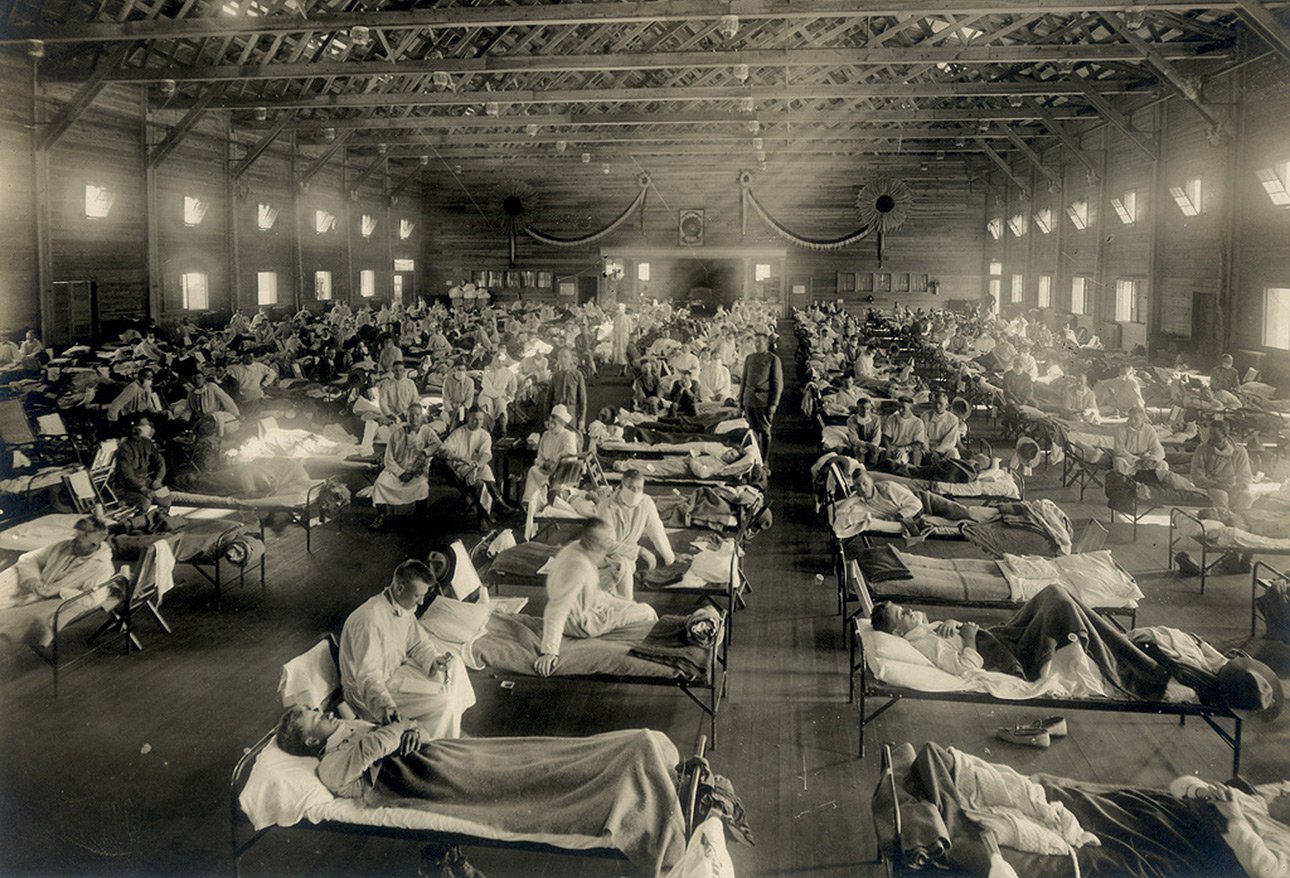
Records being very sparse back then, as far as we can tell now a good ONE-THIRD of the entire world’s population (about 500 MILLION people) caught influenza that season! The vintage photo is of a “hospital ward” full of that years’ patients .
That years “flu bug” (influenza virus) was INCREDIBLY pathogenic. In fact, it was unprecedented in history.
Incredibly, about 2.5% of those who became infected—were KILLED! That was possibly up to twenty times more than our best estimates of deaths than we would have predicted.
NOW: Pathogenicity and Mortality Rates
The death rate for Influenza since the GREAT INFLUENZA has been considerably less, not quite 0.1 percent. And these days the Center for Disease Control (CDC) keeps a lot better records and is better to be a whole lot more help in combatting epidemics.
However, still, these days 1 out of 1,000 “flu-infected” people are expected to die.
All the CDC data between 2010 and this season show: CASES: 9,200,000–35,600,000; HOSPITALIZATIONS: 140,000–710,000; DEATHS: 12,000–56,000. That’s a range of 1.5–2% hospitalizations and 0.13–0.16% deaths, in case you were wondering.
For comparison, the CDC reports THIS YEAR (so far, Feb ’18): the number of Influenza victims seeing their “provider” for influenza-like illness is 7.1%—the highest since the 2009 pandemic.
Hospitalizations: 51.4 per 100,000 in the US. And, mortality? That’s 9.7% and also higher than average.
Highest Risk Patients
THEN: Patients at Risk
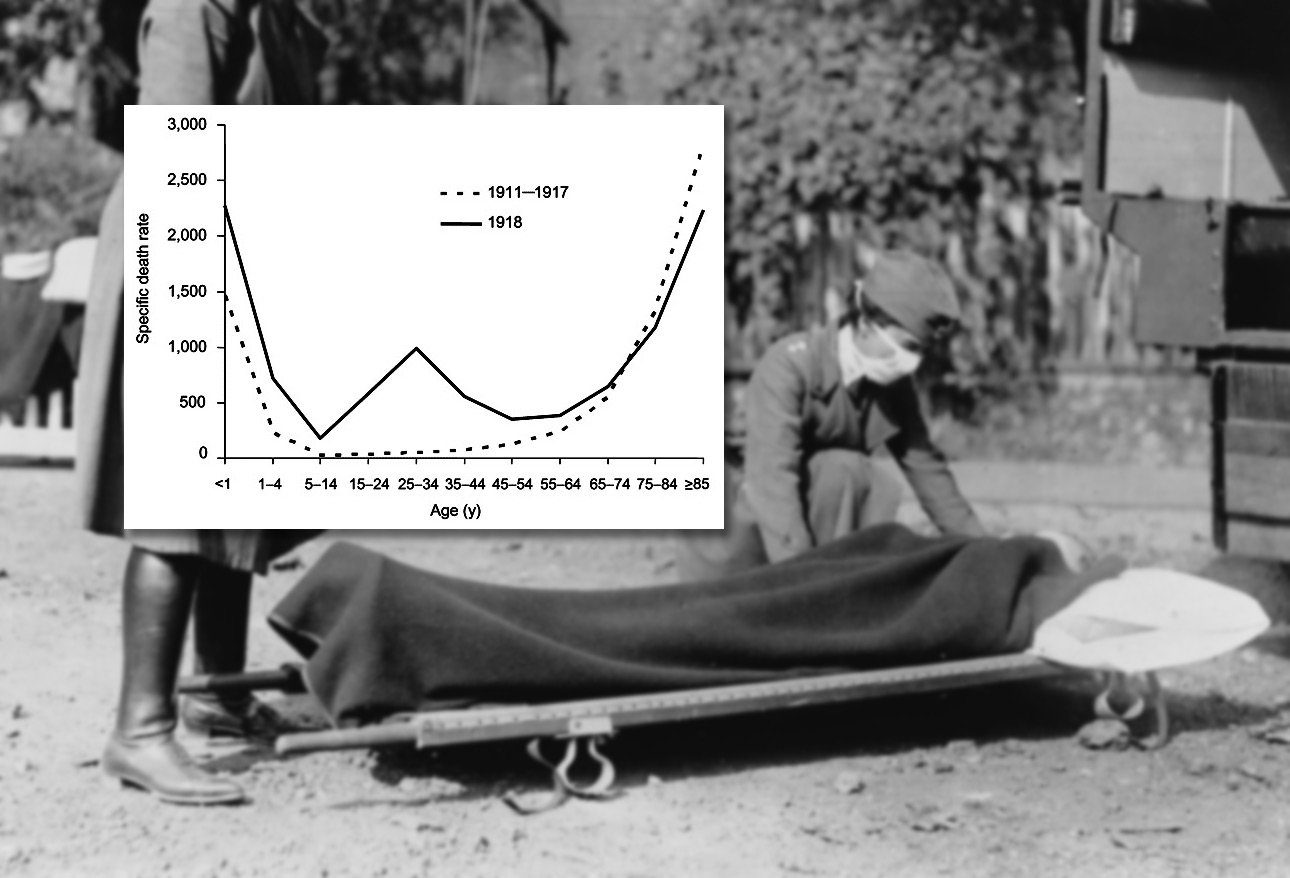
In nearly all years we know about, the “curve” of the ages of people who die of “flu” is shaped like a “U”; namely, those under 4 and those over 55 with very few in the ages in-between.
The GREAT INFLUENZA was a different story! Half of those who died were between 20 and 40 years old—the prime of life. That curve was a “W”.
That season, 15 to 34-year-olds were more than twenty times more likely to die than in any year previous—and remember, that was 12-56 THOUSAND deaths.
NOW: Patients at Risk
The CDC considers those with the highest risk for “flu” complications to be: children less than 5; adults > 65; pregnant and up to 2 weeks postpartum women; long-term care residents; Native Americans; those with chronic health conditions including immunodeficiency.
Last season (2015-16) older adults accounted for under 10% of the cases but more than 60% of the excess deaths from pneumonia or influenza.
As of Feb 3th of this season, 63 children have died from influenza and 85% of those deaths were in non-vaccinated patients.
What Causes It?
THEN: What Was Known
Something happened immediately before 1918 .
Before the GREAT INFLUENZA, “the flu” was thought a relatively unimportant 3-day fever and not life-threatening. It wasn’t even on the public health radar as a reportable disease. But not afterward by any means!
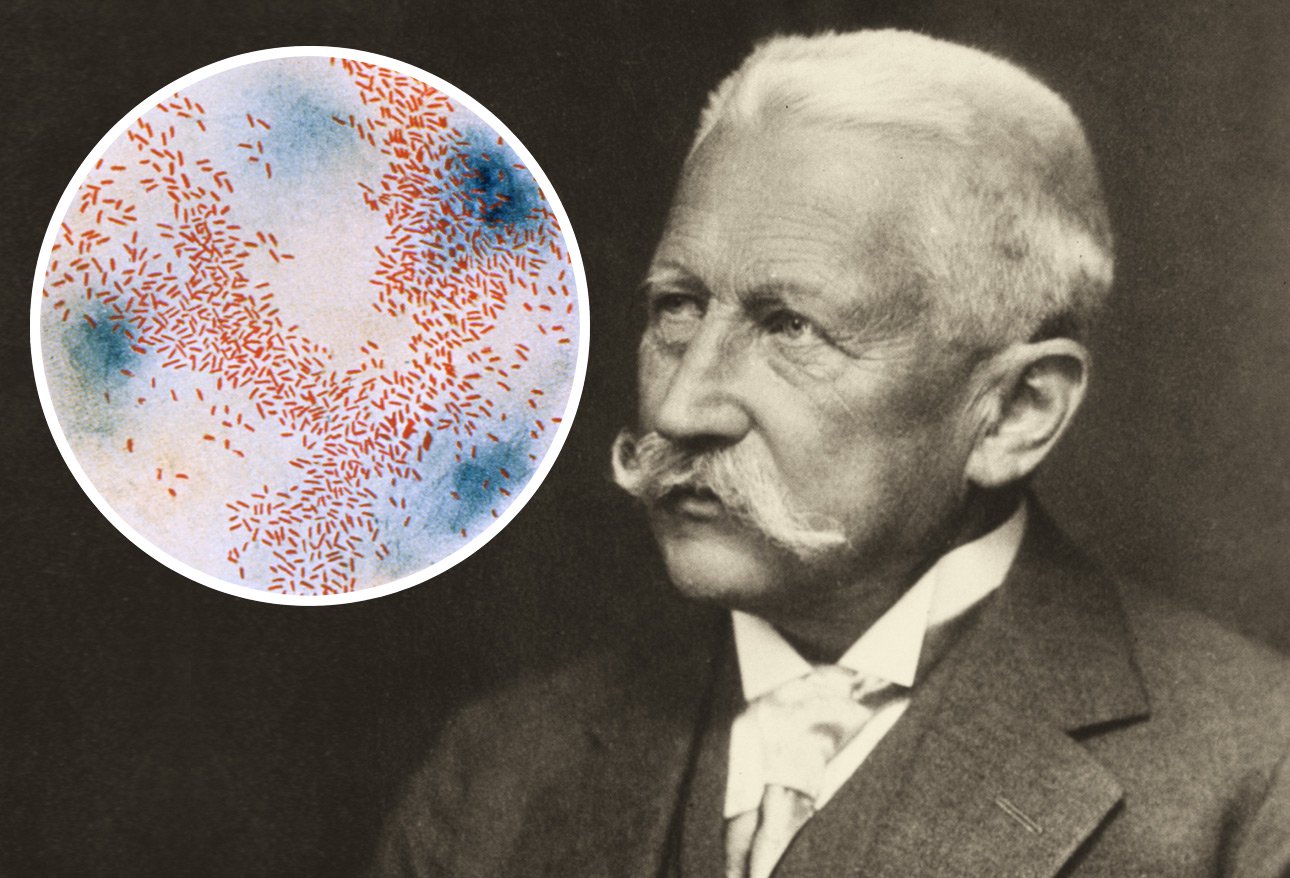
In the early 1900s the “germ theory” of disease was known and Dr. Koch had even received his Nobel Prize for developing the field of bacteriology; but, the best guess for a cause of Influenza was “Pfeiffer’s bacillus” discovered about 15 years prior by bacteriologist Richard Pfeiffer.
The “bug” was eventually characterized and named—which has been the nemesis of humanity ever since: Haemophilus influenzae, which we now know causes lots of infections EXCEPT Influenza. Unfortunately, the name has stuck.
Thousands and thousands of hours were wasted following that red-herring lead and developing serums, antitoxins and vaccines which would be totally ineffective and a waste of time. Unbelievably some were even questioning whether the disease had really been Influenza before it’s relationship to chickens and swine were realized.
We now know definitively that the GREAT INFLUENZA was due to an influenza A virus, H1N1 subtype.
NOW: What is Known
1- Influenza is a highly contagious, mild to life-threatening respiratory disease caused by the Influenza VIRUS attacking the nose, throat and sometimes the lungs.
2- The symptoms, similar to those of the routine “cold” but including myalgia and lethargy begin after a 1 to 4 day (but mostly 2) exposure to the virus.
3- Seasonal strains of the virus are ever present but extremely virulent strains emerge periodically, without (as yet) known reason.
4- Influenza attacks both animals (birds and swine) and humans and can migrate between the two.
5- Today, after a hundred years from the GREAT INFLUENZA, the strain causing the most mayhem (2017-18) is: A/H3N2.
How Is It Diagnosed?
THEN: Diagnostic Methods
At the time of the GREAT INFLUENZA its diagnosis was not only based on limited understanding of the disease but also relied mostly on clinical observation of ill-defined symptoms using ill-defined criteria.
Some descriptions of the disease included hemorrhaging, mental changes and eventually cyanosis and it was even under-diagnosed. Physicians sometimes misdiagnosed dengue, malaria, cholera, dysentery and typhoid merely due to misreading the symptoms.
NOW: Diagnostic Methods
Today, we’ve got billions of dollars worth of laboratories doing countless assays and molecular tests on viral cultures; but, still, diagnosis relies on (a little more defined) clinical symptoms and physical examinations.
There is still a problem in that all these “new-fangled” tests rely on reactions of antigens which have been made specifically to known virus types—so, they are very SPECIFIC to those virus types.
But, what if the virus changes? That makes the tests less SENSITIVE to the diagnosis of overall influenza with multiple causes—meaning that it can MISS some… a lot of it. Also, rapid tests are less effective in adults than in children—and no, we don’t know why.
An added observation of puzzling interest is that THIS season, only a fourth of the respiratory specimens tested have been positive for influenza. Something’s changed… again.
How Is It Spread?
THEN: Known Influenza Propagation
What happens when people are scared, don’t know why and nobody’s giving them any way to prevent their danger? They start “inventing” their own “causes” and “cures” making them exquisitely vulnerable to charlatans, scams and pet prejudices (think Salem).
Let’s see: Influenza spread from person to person, had 3-6 day incubation, went hand to mouth or nose, objects could become “infected” with whatever it was and contaminate when touched.
Also, it obviously was exceptionally contagious and the crowded conditions after WWI, the centers for displaced people and army barracks for example, were “hot beds” of the disease.
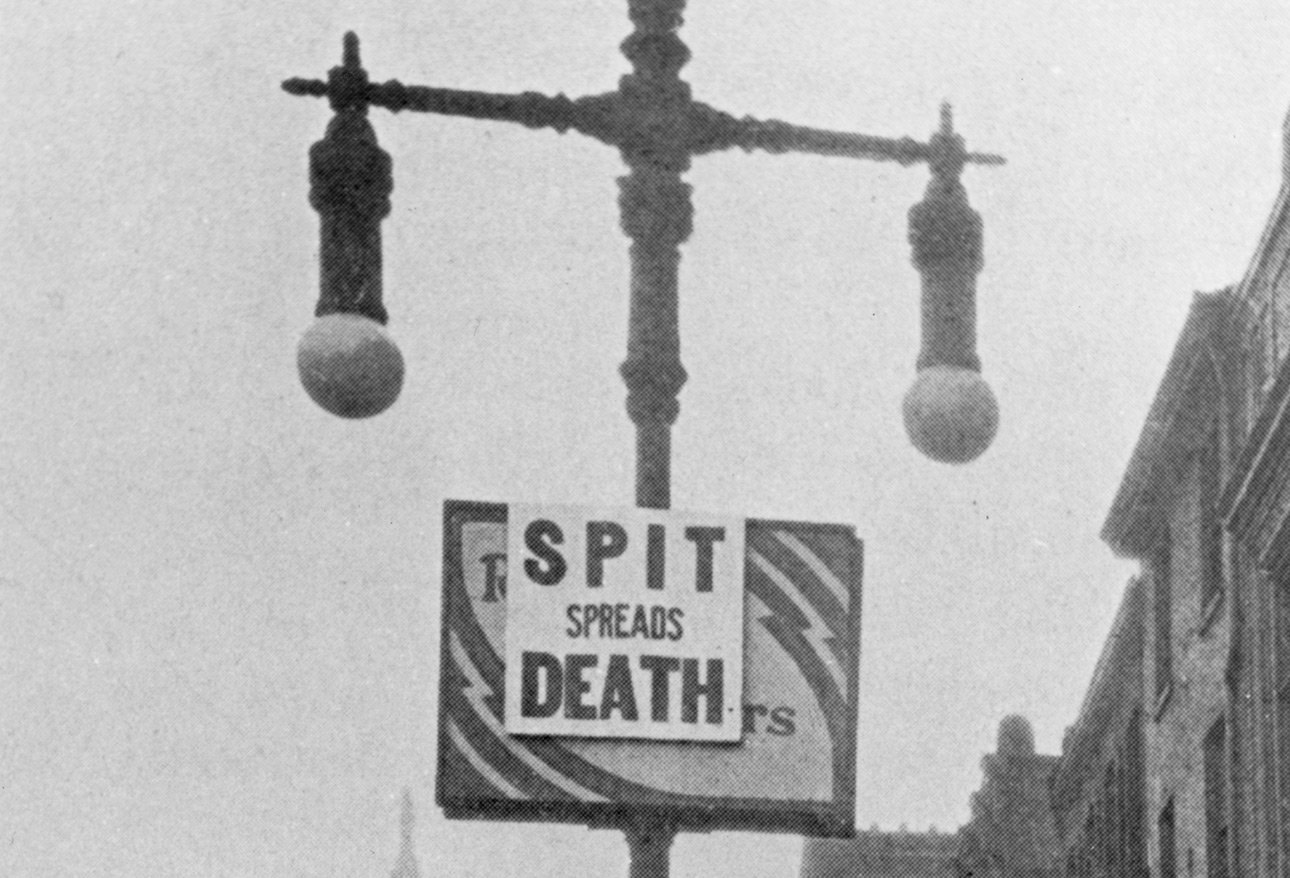
Frightened people were inflamed further by the media of the time, such as it was, and signs similar to this (Spit Spreads Death) were posted all over—anyone caught spitting was arrested or fined.
NOW: Known Influenza Propagation
Today we know:
1- Influenza virus spreads, up to 6 feet, with every cough, sneeze (or even talking) of an infected person;
2- Spread can even come from contaminated objects;
3- Precautions should be taken by covering the nose and throat when coughing or sneezing (with something besides the hands) IN ADDITION to frequent hand washing;
4- Healthy adults can shed the virus one whole day BEFORE symptoms occur and 7 days after becoming sick;
5- Children transmit the virus even longer than that; and,
6- Amazingly, some infected persons shed their virus WITHOUT even having any symptoms at all!
How Do We Treat It?
THEN: Treatment Options

Let’s face it. During the worst epidemic of all time doctors were completely caught with their options down; and the good ones were embarrassed and ashamed about it. A leading pathologist of the time, William Welch, wrote: this pandemic “will forever be a great shadow cast upon the medical profession.”
In 1918 what they were doing was: bleeding, cupping, purgatives, cardiac stimulants and… many even more outlandish, bizarre and completely worthless treatments. Physicians were completely powerless to alter or prevent the pandemic.
While the public was falling scam to such fraudulent remedies as camphor, garlic and gargling, physicians couldn’t do more than relieve at least some of its symptoms with aspirin, oxygen and morphine. “They watched helplessly as countless young, otherwise healthy patients succumbed to the disease.”
NOW: Treatment Options
Today, we do have some antiviral drugs with limited action and usefulness. They became available in the mid 60s and have helped at least “change the landscape” a bit in the treatment. They “possibly” are effective in reducing mortality in those hospitalized and they “might” shorten symptom duration up to one day in the general population.
A couple drugs might be effective at reducing secondary transmission; BUT, they are very expensive (surprise, surprise) AND they don’t work well after two days with symptoms.
Can We Prevent It?
THEN: Preventive Measures
There was nothing else available so it soon became clear that avoiding exposure to sick people was the only option to prevent getting sick; but, how can an entire population (most living hand to mouth in a subsistence living) be physically isolated?
This was the time when paper cups were invented and became popular. And community leaders took measures into their own hands with rules, regulations and fines. The parable of the “Good Samaritan was excruciatingly put to the test”; and, if you “came down with it” you really discovered who your friends were.
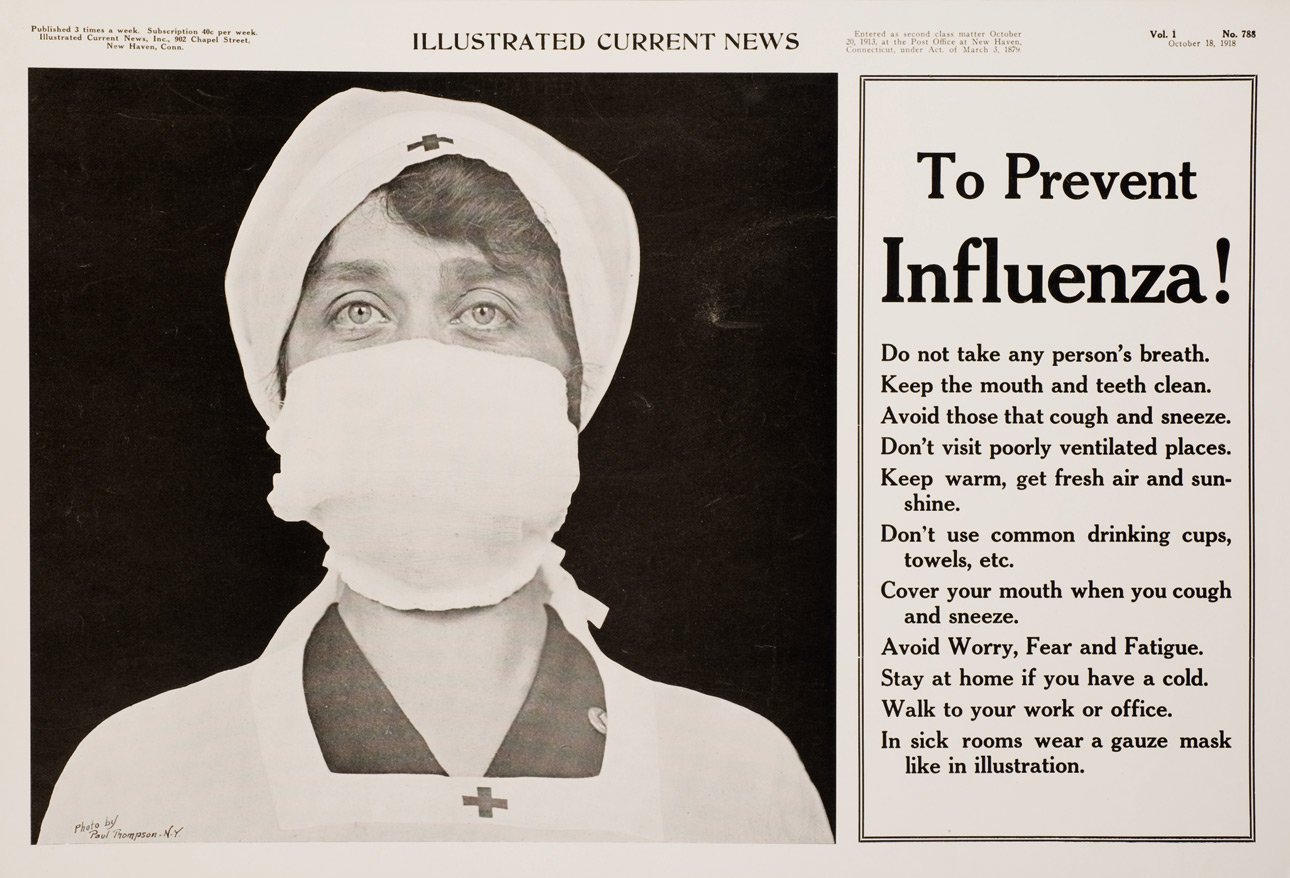
The advertisement to the right enumerates some of the more realistic preventive measures advocated in 1918 (click to enlarge). Public gatherings were banned.
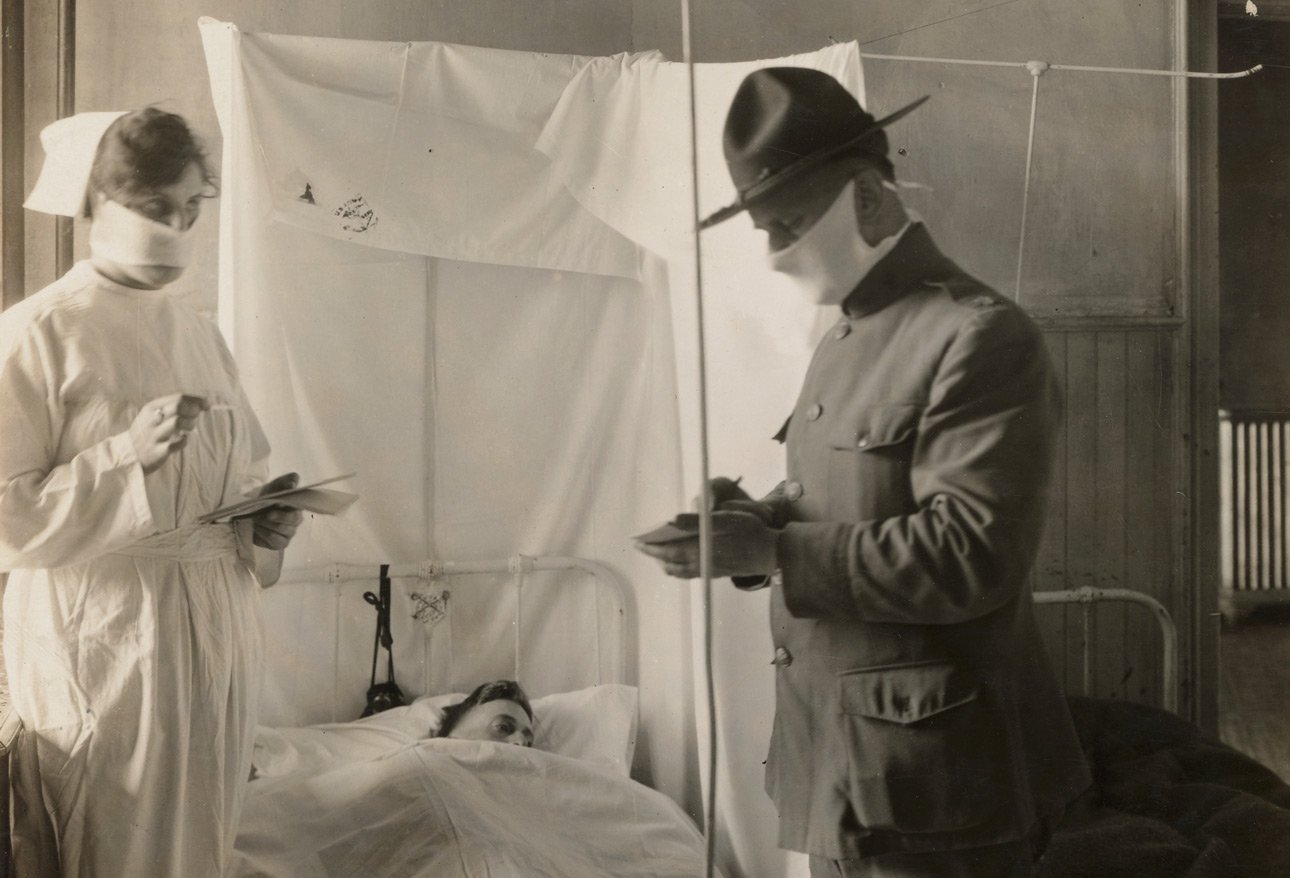
Additionally, face masks were distributed to the public and made mandatory. They became the de Facto symbol of the GREAT INFLUENZA—even though we now know the gauze of that day is pretty much useless in preventing viral transmission.
The media and entrepreneurs came out in abundance to make their wealth off of the inflicted. Before the hype was over, young healthy people with jobs and money were going to great lengths to avoid dying in the epidemic.
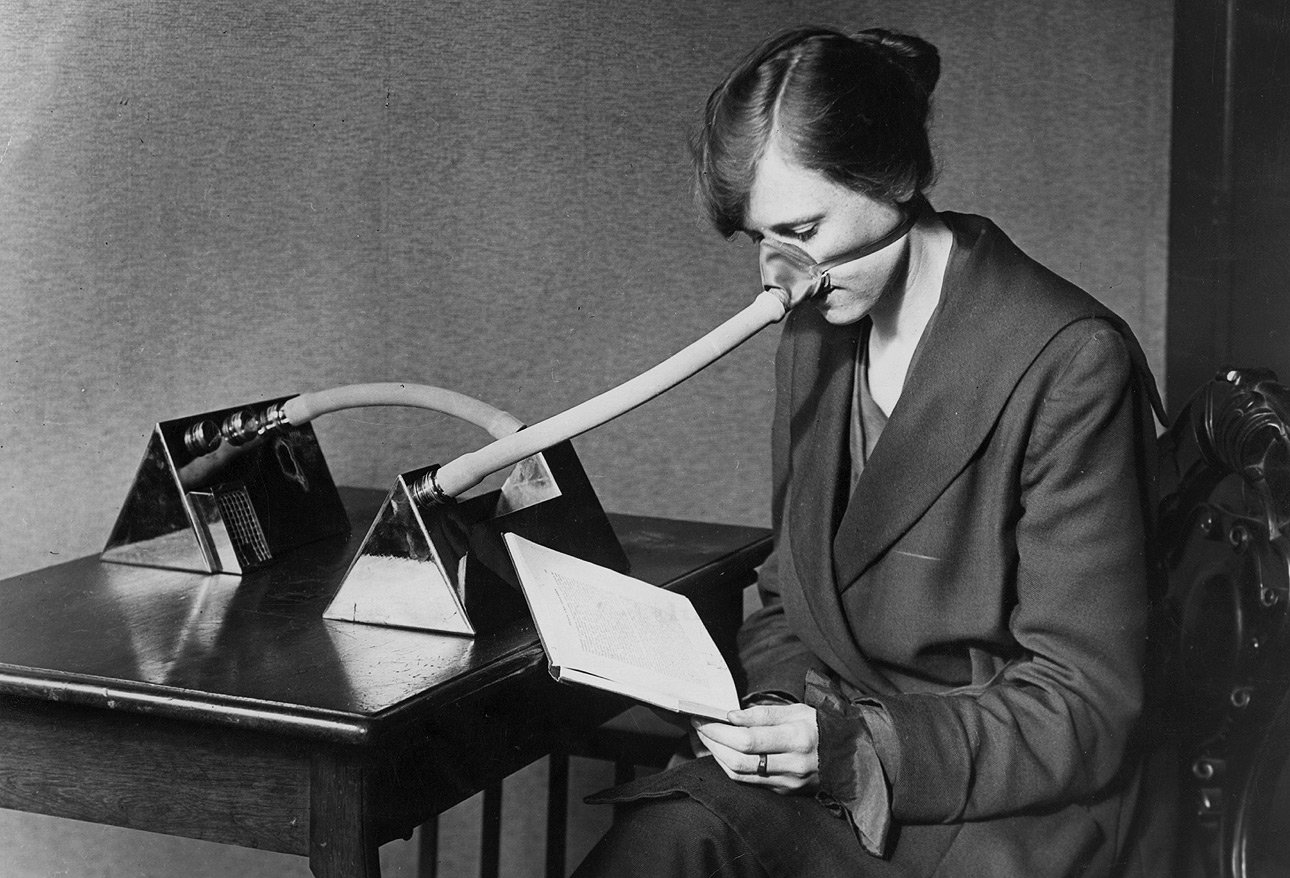
An advertisement of the day is for a “flu nozzle” designed to prevent infection while sitting at your desk—ostensibly to be used by people whose jobs required them to be in contact with the populace.
It passed air through tubes and chambers, which would merely by construction cause micro-droplets of expelled mucous to drop out of circulation. But, you can see that its volume would build up carbon dioxide so readily the wearer would be poisoned unless they removed it or alternately breathed out through the mouth.
Young adults seemed the “target” for this new vengeful “bug” and speculation as to why was rampant. All the theories revolved around prior exposure and undeveloped antibodies of that cohort, which wasn’t too far from the truth.
It did get a lot of people thinking about pandemics, patterns, vaccinations, immunity and public health.
NOW: Preventive Measures
What have we got now? Well, just a little more than a hundred years ago… but just a little. I’ve already mentioned antiviral medications which sort of take the “sting” and inevitability out of severe infections; but, obviously, not the mortality.
And, we’ve got better gauze masks (or their equivalent) but don’t yet have direct proof that they are any more effective than those of yesteryear and too many Kardashian-like image concerns to get US citizens to wear them.
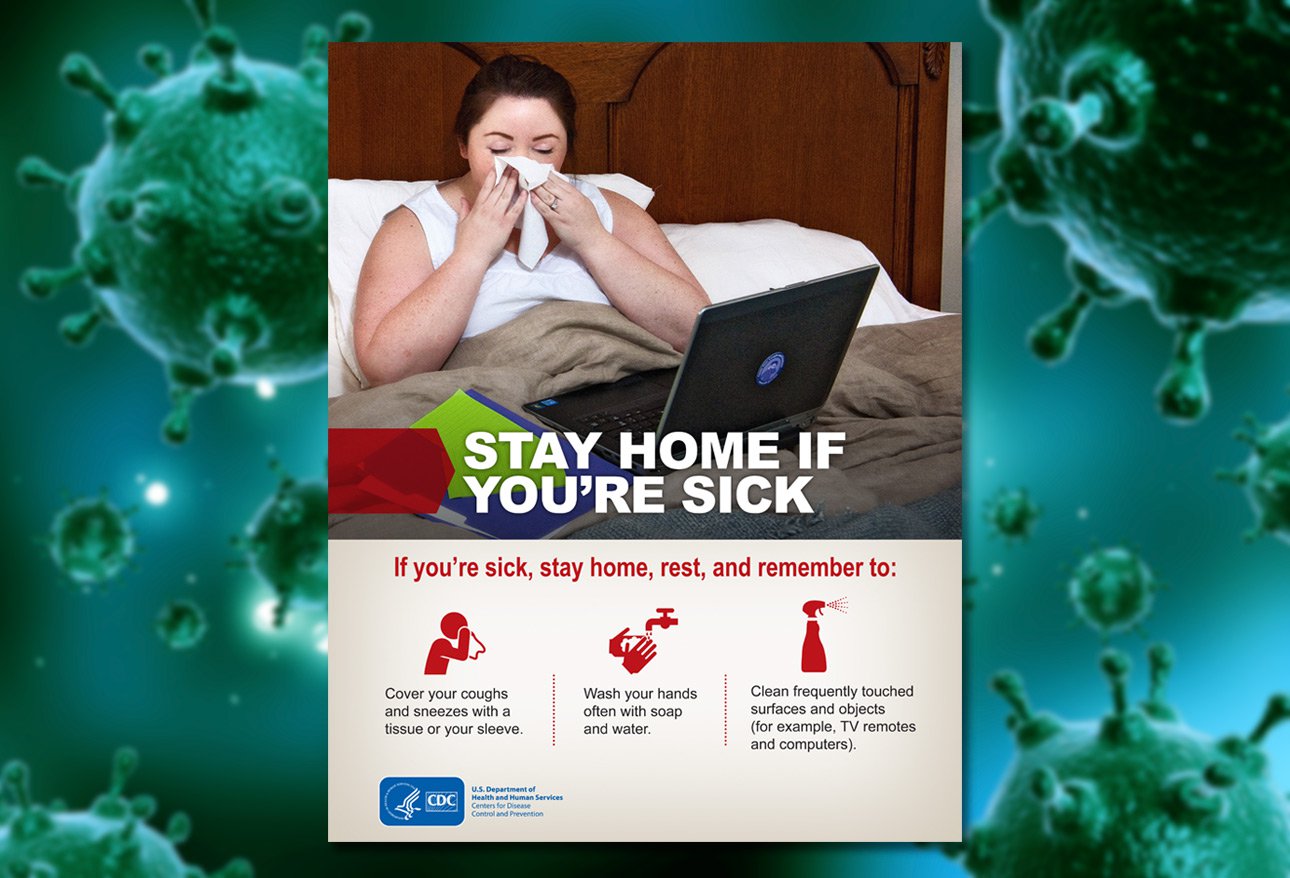
Largely however, the preventive hygiene measures we publish today are kin to those of yesteryear, with just a few upgrades. For example, school children of today are taught to “cover your mouth with your elbow” instead of with their hands. The hardest thing to penetrate into people’s minds is to “stay home if you’re sick!”
THEY didn’t know about frequent handwashing being a critical measure like we do today; nor did they have the clout to get so many businesses to give out all the hand-wipes.
THEY also didn’t have the nightmare of the international mobility and transportation that we have now. How are we seeming to control the chaos and, until now, avoid every year turning into a pandemic? The answer: Flu Shots.
Twenty-first century preventive measures also encompass a sophisticated global network of surveillance, monitoring, and reporting, such as FluView and FluView Interactive, operated by CDC’s Epidemiology and Prevention Branch and the World Health Organization’s Global Influenza Surveillance and Response System
Do Vaccines Help, Really?
THEN: Influenza Vaccines
It should be obvious to you that back THEN there was no “flu shot” even though they did know and understood the concept of vaccines. They still had no clue about the Influenza virus.
That didn’t stop them from creating many different vaccines, antitoxins and antisera, mainly against Bacillus influenzae and pneumococci, even though the suspicion was that there was something else which was the culprit.
Their “vaccines” were given desperately to save lives, or to the military and to others who desired and could afford them. None of them worked though.
NOW: Influenza Vaccines
Having actually lived through the GREAT INFLUENZA, so still seeing it clearly in the rear-view mirror, in 1933 scientists finally isolated the influenza A virus and by the end of WWII a vaccine had already been used successfully to prevent flu in US troops! Vaccination of civilians could begin.

That lead rapidly to more and more discoveries about the issue; but, unfortunately, the discoveries were all too public so learning that last years vaccine wasn’t as effective on this years virus discouraged some.
There’s a hemagglutinin coating on the virus which is capable of mutating so readily that even the body can’t develop natural antibodies to it. Just like the thousands of “cold” viruses which we can catch one after the other.
So, how is a flu vaccine made then if even the body can’t do it? That’s where South America and other continents “down under” come to the aid of us in the north (and vice versa). The CDC and others carefully surveil the “southern disease” during their winter before it hits us and make vaccinations to them—we do the same in the other direction for them.
Even so, mutation can occur as it crosses the border, like we think happened in 2914, or as the vaccine is grown in the eggs during manufacture, like we think happened in 2016. In those years vaccine effectiveness is less; BUT, we have learned that it still IS ENOUGH to modify the severity of those who become infected AND to prevent pandemics.
A yearly flu vaccine is considered the most effective way to prevent influenza despite the problems.
Public Attitudes
THEN: Attitudes Toward Influenza
People of 1918 might have heard about the “Russian flu” that occurred 30 years in their past; but, the GREAT INFLUENZA they were experiencing was completely new to them. Before influenza wasn’t on their minds as a threat—especially since they were focused on World War One.
Now things had changed for them, the second of three “waves” of deaths had begun, dead were piling up (literally) and medical science couldn’t protect them. Making it all the worse was the fact that those caring for the sick (nurses, physicians, parents and friends) were dying at the same rate as their patients!

Fear caused the well to refuse to go to work and be unwilling to help one another (a personality trait here-to-fore completely foreign to the country). Without donning masks, people were refused entry to public transportation.
Government attempts to boost morale with such messages as “There is no cause for alarm!” and “Don’t get scared!” had the opposite effect, to no one’s surprise.
THEN, once the pandemic had run its course, and perhaps associating it with a war they wished to forget, people seemed anxious to bury the memory; until…
NOW: Attitudes Toward Influenza
…TODAY when they are so uninformed that they’ve got the leisure to be too disinterested to obtain flu shots.
Attitudes have evolved both through discovery and complacency and the fear and panic the GREAT INFLUENZA generated have been consigned to history books .
Today, the data shows that only about half of the US population considers influenza enough of a threat to suffer the inconvenience to get a flu shot. In 2015-16 coverage was only 46% among those over 6 months; even though those older than 65 (who took the threat more seriously) had a rate of 63%.
The reasons: not a perceived need (28%), didn’t “get around to it” (16%), “not believing in flu shots” (14%) and thinking the “risk is greater than the disease” (14%).
The pandemic of 2009 did trigger a bit of widespread alarm and the current death rate from Influenza seems to be having an effect as well. The 2017-18 season has seen hospitals at the breaking point, antiviral shortages, school closures and rising deaths.
Understandably there is a bit of an alarm… perhaps there is hope yet. Remember, those who don’t know their own history are destined to re-live it.