
What’s Eating You? Bedbugs, Mites and Lice
There are lots and lots of things that cause rashes in children and we’ve spoken about them several times before. There are fewer problems that cause rashes that itch and less caused by things that bite— although that’s still more than in a world I would create… if it were me.
Bugs that bite, rashes that itch
Now that the injuries and poison ivy are taking a short sabbatical here in the US other things are reminding us that they’re still around. Here is the latest information on the top three problems we see (in the U.S.) which cause itching rashes in children: bedbugs, mites and lice.
It’s true that these parasites thrive in conditions of overcrowding and decreased sanitation; but, those of ALL socioeconomic backgrounds are at risk for infestation causing substantial skin and psychological discomfort.
A Rash That Itches
Frankly, these three issues are a bit more difficult for parents to diagnose because, while things like poison ivy seem easy to accept as a cause, the fact that your child is being “eaten by a bug” is something that most of us think just couldn’t happen in our house.
What the rash looks like depends upon what style the little gremlin uses to feed and what type of substance the suckers inject into the kid. Of course, having the wound later become secondarily infected by a bacteria or fungus changes how they look too.
Bites from bedbugs can lead to a hypersensitivity reaction called “papular urticaria” (see below); Lice, on the other hand, commonly cause their “rash” from the intense itching, especially at night, and scratching; and, mites (scabies etc.) produce linear burrows under the skin.
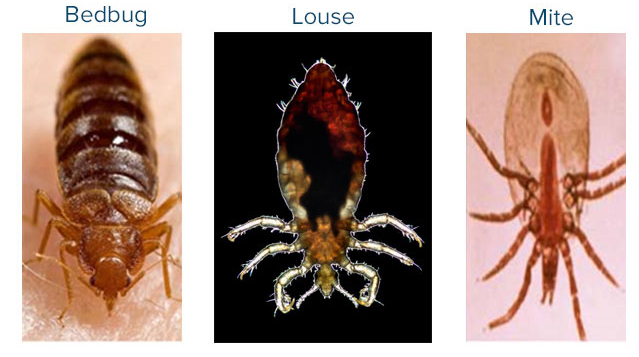
Bed Bugs

Bedbugs are under a half-inch long and reddish brown. They are found in furniture, bed frames, mattresses, between floorboards, behind peeling paint and other small places of clutter.
They feed at night, especially just before dawn, and find their prey by body heat, exhaled carbon dioxide, vibration, sweat and odor. Like mosquitoes, they bite and inject anticoagulant and other “stuff” into the skin before sticking their mouth into capillaries which cause them to fill with blood and change colors, also like mosquitoes.
The bites are painless but with the repeated bites along a track the body’s resulting allergic reaction to all the injected “stuff” isn’t—and the things intensely itch. The photo on the left shows the papular urticaria of bedbug bites along an arm.
Treatment is supportive including any secondary infection that occurs. Bedbugs can be eliminated with Permethrin based insecticides, baited traps, special bedbug-free beds and bed nets along with correcting/replacing any clutter, worn/old frames and/or mattresses and chipped paint.
The thing is though, the little suckers have been known to climb other objects and then fall down onto the bed.
Lice

These little troublemakers can be either “suckers” or “chewers” but only the “suckers” purposefully seek out humans to infest. And the “suckers” some in three flavors: Pediculus humanus “capitus” (head louse); “corporus” (body louse); and, “pubis” (pubic louse or ‘crabs’).
They all do a body damage by piercing and ingesting blood but only the body louse is known to spread other diseases (typhus, trench fever, and relapsing fever). The photo shows a female louse (singular form), but after they lay eggs (nits) that hatch and go through larvae stages there are lots of lice (plural form).
Body lice infest clothing, laying eggs on fibers in fabric seams which make them controllable by washing and changing clothing often; unfortunately not practical for homeless persons making them particularly susceptible.
Both head lice and pubic lice infest hair and lay their eggs on the base of the fibers. The two look different with the head louse being longer and the pubic louse shorter and stubbier. People don’t like admitting they have either so don’t talk about it with their close contacts allowing others to be infested in epidemic fashion.

Pubic lice are generally spread through sexual contact so doctors use them as a “marker” to look for other sexually transmitted diseases as well. And, believe it or not, enterprising public health officers have extracted DNA from pubic lice in rape victims and identified their attackers. And just as oddly, Lice found on the eyelashes are typically pubic lice rather than head lice.
Children can be without symptoms when they get head lice, but adults almost always have intense itching (pruritus). There may be swollen lymph nodes in the area, there may be impetigo (like in the photo), there usually is excoriations (scratches) from the itching with dark specks of louse feces, nits, and adult lice. Oh, and it’s most prevalent on scalp in back of the ears.
Body lice can be found on the seams of the patients clothing (if the doctor bothers to look) and often have produced bruise-like spots on the skin. Pubic lice, like body lice, are usually observable with the naked eye; if someone gets close enough to look, they can see both adult lice and nits.
Treatment of lice infestation is typically approached as a community-wide problem; otherwise, reinfestation will reoccur. All persons potentially infectable must limit the sharing of, or contact between, personal objects, such as combs, brushes, and clothing. That is known as “fomite control” and is critical to the eradication.
Pediculicides, such as permethrin and malathion, can be used to kill adult lice, but young nits are immune to neurotoxic agents because they do not have nervous systems. In that case specialty combs with very tight bristles can help remove nits from hair follicles.
For the treatment of body lice, removal of infested clothing and laundering in hot water, ironing with a hot iron, and drying in a hot dryer are all effective; but you can’t merely rely on any of the machines available today to take care of everything for you—you’ve got to personally make your best effort for longer than you want to do it. Topical agents may also be applied to clothing.
Mites
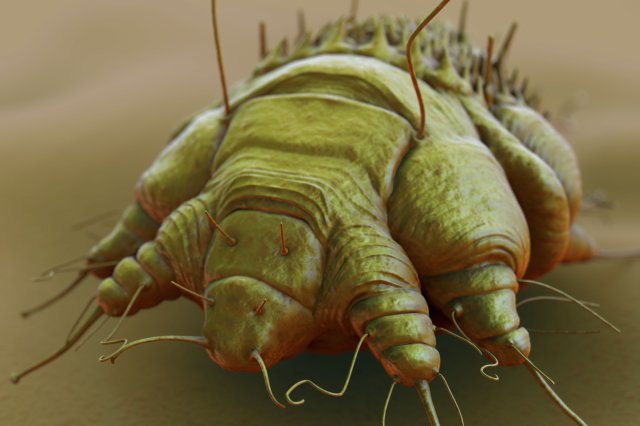
Mites are in the class with spiders because they have eight legs. Fortunately only a few of the 48,000 species clinically involve humans—but that’s more than enough! The disease it causes, Scabies, is a global health problem which flourishes in areas of overcrowding and poor public education and too often is delayed in diagnosis and treatment.
Living their lives in 30-day cycles under human skin, eggs hatch into larvae which feed on digested tissue leaving fecal matter behind them in their burrows as they migrate. Eventually they mature into adults which lay eggs and the cycle begins again (photo on left).

By the time diagnosis is made there are usually 10-100 mites already burrowing but immunocompromised children may harbor more than a million with intense itching due to a hypersensitivity reaction and/or a super-infection.
They can survive on fomites such as bedding and clothing for up to 3 days but transmission between individuals is with direct and prolonged contact (skin-to-skin and sexual) with an infected person.
Children will show mites on the face, scalp, neck, palms and soles in a diffuse manner and less often in the adult pattern which is the web spaces of the hands, top of feet, axillae, elbows, waist, buttocks and genitalia.
Catching it early in the primary stage means small papules, vesicles and burrows but secondary lesions increase due to rubbing and scratching. Doctors who have seen them before might be able to diagnose by actually seeing evidence of their life-cycle; however, looking at skin-scrapings under a microscope will reveal the actual mites or their larvae, ova or fecal pellets.
If the common delay in diagnosis wasn’t enough of a problem, getting patients to follow through with adequate treatment is just as big an issue. You CANNOT do it “almost” or “half-way” or leave out other members of the household. ALL members and close personal contacts must be treated, thoroughly to completion! Skin-to-skin contact isn’t usual for school-aged children (unless they are wrestlers); but, that’s not the case for toddlers and preschoolers. Daycare centers are often the source of the mites.

Treatment is with scabicidal agents (Permethrin cream, oral ivermectin, lindane cream/lotion), anti-itching medication and sometimes antibiotics; again, for ALL household members and close personal contacts. The creams and lotions must be applied on ALL and EVERY skin surface except, obviously, in the eyes, nose, mouth, tip of the penis or vagina. On older children you can come fairly close to those sensitive structures but on babies and toddlers who can’t be trusted you need to apply leaving a margin.
If you think the photo (I found on the internet) is a good application it IS NOT. No gaps should be left. ALL surface areas means just that: every single whit; into the hairline; in all the “cracks” and folds; between digits, buttocks and legs. Eggs can be anywhere and I’ve seen all of those locations be the reason for treatment failure. Mites will migrate into unapplied areas.
Clothing, linens, and towels must be laundered on the hottest setting (turn off the valve to the cold water if you need to). The same thing with the dryer, the longest and hottest setting practical.
AND you should repeat the treatment in 5-7 days, to catch those that hadn’t hatched yet, THEN see your doctor for reevaluation 2-4 weeks after treatment to ascertain eradication of the mites. I need to say that one of the reasons doctors are concerned is that we are now seeing infestations which DON’T respond to the common agents anymore and some of the more powerful agents can have neurological side-effects.
Just DON’T do it half-way the first time around because it gets harder with every attempt!
7 Posts in Bug Bites (bugbites) Series
- Part 2 - 33 things about bug bites: fleas, bed bugs, spiders, Zika, Dengue and Ehrlichiosis. – 28 Mar 2018
- Part 1 - 33 things about bug bites: Ants, Chiggers, Ticks – 23 Mar 2018
- Ticks and Fleas – 11 Dec 2016
- Bed bugs, Mites and Lice – 7 Dec 2016
- Mosquitos and their illnesses – 23 Jun 2016
- Scabies is coming back! – 27 Oct 2014
- Bug Bites Series: Intro/Index – 15 Oct 2014
Advertisement by Google
(sorry, only few pages have ads)