
Can We CURE AIDS? No and Yes
Can we CURE AIDS? Well, pretty much always no. But hope for a cure has never been brighter than now, with two infants well on their way to a cure – one of them now three years old, if you can believe it, and disease free off meds.
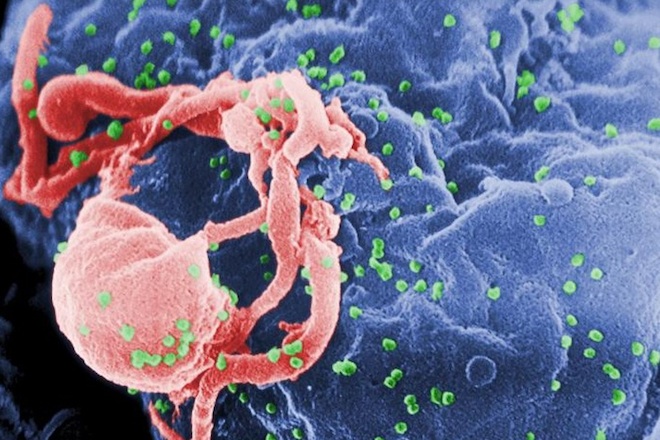
Tiny buds of HIV virus releasing from cell where they are replicatingI want to tell you about a report from the 2014 Conference on Retroviruses and Opportunistic Infections (March 5, 2014) where a speaker gave an update on the two babies now who have been born with aids and become “virus free” after their pediatricians used heavy doses of the standard AIDS medicines available today.
As we all know, there is a problem with making statements using absolutes – you never say never – and the rule is probably even more important when you’re talking about those stinking, little viruses.
Right now laboratories can only detect down to about 20 virii (single virus particles) per milliliter of plasma. So, theoretically, a person feasibly could have 18 virii per milliliter and avoid detection; which is why you hear the term “functionally cured” used a lot – “Cured for all intents and purposes,” or “cured as far as we can tell.”
AIDS in Infants
Of the eight babies born in the U.S. every minute (4.25 million/year) only a few hundred are born infected with the AIDS virus thanks to antiviral treatment in pregnant mothers. Women in Africa are not so lucky. Their 75 births per minute yield over 300,000 babies born with AIDS. No small issue!
 Princess Diana, the first high profile celebrity to be photographed touching a person infected with the HIV virus holds a Brazilian baby with the diseaseNot all babies born of HIV positive moms get infected, only about 15-45%. And with methods already in place, that number can be reduced to more like 1% — if medicines and care were available and complied with.
Princess Diana, the first high profile celebrity to be photographed touching a person infected with the HIV virus holds a Brazilian baby with the diseaseNot all babies born of HIV positive moms get infected, only about 15-45%. And with methods already in place, that number can be reduced to more like 1% — if medicines and care were available and complied with.
And, unlike in adults, with babies you almost know exactly the time they were infected – usually at birth; which, as it turns out, is the optimal time to begin treatment.
“Cures” in Infants
It would be almost impossible for an AIDS infected woman to deliver in a U.S. hospital and not be on treatment (which of course can’t be claimed for home and birthing centers); so, testing and treatment of an infant would be initiated almost immediately as was the case of the Mississippi infant three years ago.
That infant had been born to a very recently diagnosed AIDS patient who had not yet received any medication. At 30 hours of age, before lab tests confirmed infection, the baby was put on a 3-drug “cocktail” of standard anti-AIDS drugs. (If the mother had already been on medication the baby would probably have only received the standard one-drug medication)
The test were eventually shown to be positive so the full “cocktail” was continued. At 29 days the baby had responded to the point that no viral load was detectable – all the tests were negative.
For some reason which wasn’t reported, the mother stopped treating the child at about 18 months of age.
Months later, on a follow-up visit, the discontinuance was noted and a complete blood panel was analyzed in order to not only re-check the diagnosis but to see how much further the baby’s disease had progressed.
 Tiny buds of HIV virus releasing from cell where they are replicatingTo everyone’s surprise, no actual virus particles could be found in the baby’s plasma and no apparent reservoirs were found. Even more sophisticated testing showed that such a miniscule amount of HIV DNA had incorporated into the genetic material of the baby that it was just barely detectable and only one, single HIV RNA particle was found.
Tiny buds of HIV virus releasing from cell where they are replicatingTo everyone’s surprise, no actual virus particles could be found in the baby’s plasma and no apparent reservoirs were found. Even more sophisticated testing showed that such a miniscule amount of HIV DNA had incorporated into the genetic material of the baby that it was just barely detectable and only one, single HIV RNA particle was found.
The baby was declared “functionally cured” and the doctors made headlines by reporting it. The purpose of anti-retroviral therapy is to block viral replication in the blood. Because there was no detectable virus in the blood after 10 months of no medication there was no virus to block and the team advised not to restart medication.
Really, really close follow-up shows that still after 39 months of age (21 months after stopping meds) the baby has “undetectable plasma viremia (<20 copies/mL) and normal CD4+ and CD8+ T-cell counts." And, “The child remains in remission and there’s no replication combinant T-cell reservoir detectable to date.”
A Second Baby
Now a second baby in Los Angeles County California is perhaps beginning a similar course. The mother had AIDS and a “high viral load” in her blood. She had been prescribed antiretrovirals (AIDS medications) but had not taken them consistently.
By four hours after birth the doctors knew the baby had a positive peripheral blood (i.e. not the chord blood which might have been contaminated by the mothers blood) HIV DNA polymerase chain reaction – the test used to confirm an AIDS infection. Anti AIDS medicine was begun immediately at 4 hours of age.
By 36 hours of age the doctors had actual quantified reports that “the baby had 217 copies per mL HIV RNA levels.” By the sixth day of life HIV DNA testing was negative and now (Mar 2014) viral levels continue to be negative.
 Infant infected with the AIDS virus receiving anti-retroviral medication.The baby has not, at this date, been taken off medicines.
Infant infected with the AIDS virus receiving anti-retroviral medication.The baby has not, at this date, been taken off medicines.
Forthcoming Studies
These two cases have, as you can imagine, stirred the medical community a bit and within a few months (Mar 2014) clinical research will begin both in the U.S. and internationally to test the effects of very early treatment in HIV-infected infants.
Another part of the research will be to gather physicians’ experience from around the world who have treated babies with HIV very early – it just may be that there have been other “cures” or “near cures” without being realized or reported.
The longer you have HIV, the greater the chance of having a substantial reservoir of virus growth in your body which has, to date, precluded “cures” in adults.
The goal of therapy is to decrease the size of that ultimate reservoir and it appears that in those cases where medication is begun extremely early at least a “functional cure” is possible.
It’s a case where we wish we already had gathered the data and experience from around the world and knew what people had found; because, it’s awfully “gutsy” to stop a baby’s AIDS medicine.
How good is good and just how cured is cured. That’s the next step isn’t it? What are the guidelines we can use to decide when to stop your babies medicine?
[2014 Conference on Retroviruses and Opportunistic Infections (CROI). Presented March 5, 2014.]