
Child Diseases Parents Should All Know About – Part 4
We’re now well into the series about Child Diseases Parents Should Know, part four in fact.
What we’re really doing is taking a nostalgic look at the old “second brain” binder which I (along with every other pediatric resident in the world) kept during my four years of medical school and years of pediatric training.
We carried them incessantly, used them constantly and experienced separation anxiety whenever we were parted.
As a “journal,” of sort, about our experiences, they all usually ended up as a list of the “commonly common” diseases afflicting the children of the area.
Still More Childhood Diseases To Know
Rotavirus (Diarrhea) and Kawasaki Disease
In In part 1 we talked about Croup and Bronchiolitis. In part 2, ear infections and “glue” ear. And Part 3 discussed Hand, Foot and Mouth Disease, Conjunctivitis and Fifth Disease.
Today, let’s tackle the old and the new (ish).
Rotavirus (Diarrhea)
Rotavirii (Latin plural for rotavirus) cause diarrhea (or for you Brit’s Diarrhoea) which can be fairly watery, prolonged and sometimes associated with vomiting. Nothing going in and “everything” coming out can be dangerous, especially for little ones.
The virus seems to be everywhere and is a leading cause of death in developing countries – again related to hygiene and contaminated food stuffs. Pretty much everyone has it at least once before they are five, usually in the winter and spring.
There is a vaccination available against the virus which can be used where the disease is endemic. Prevention is better than treatment – did I mention hand washing and clean food preparation? Once contracted, treatment is with electrolyte solutions and hydration.
Seek medical attention if vomiting prevents treatment orally, if it lasts longer than 24 hours or the baby looks dehydrated (dark or infrequent urine, chapped lips, elastic skin, loss of tears, sticky tongue, sunken eyes, etc.).
Kawasaki disease
 Few diseases effect the hand like Kawasaki SyndromeJust because a disease is only recently described (late ’60s) and is still of unknown cause doesn’t stop medical types from writing about it – a lot! Luckily it’s not too common because it’s a real bear to diagnose.
Few diseases effect the hand like Kawasaki SyndromeJust because a disease is only recently described (late ’60s) and is still of unknown cause doesn’t stop medical types from writing about it – a lot! Luckily it’s not too common because it’s a real bear to diagnose.
Whatever causes Kawasaki’s Disease (Mucocutaneous Lymph Node Syndrome – MCLNS) seems to prefer boys, under five in Japan (where it was first described); but it’s not above maligning us Gaijin’s too.
There are over 4,000 cases in U.S. hospitals each year and it’s got its own support group and web sites because the rare heart complications of untreated cases are so severe.
It’s an auto-immune disease with an exasperatingly illusive environmental trigger – the fool thing has stayed dominant in the orient BUT causes outbreaks in Hawaii and San Diego RELATED TO TRADE WINDS AND EL NINO! No kidding!
The reason it’s a bear to diagnose is: 1) We don’t see a lot in the US so don’t think about it much; and 2) It acts like so many other problems that they are diagnosed and treated first.
This needs to have a full article on its own, which I will do in the future, but the best thing I can do right now is to get more people thinking about it by “deputizing” all of you and tell you what to be on the look out for.
Phase One
- Fever often higher than 102.2 F (39 C) and lasting more than five days
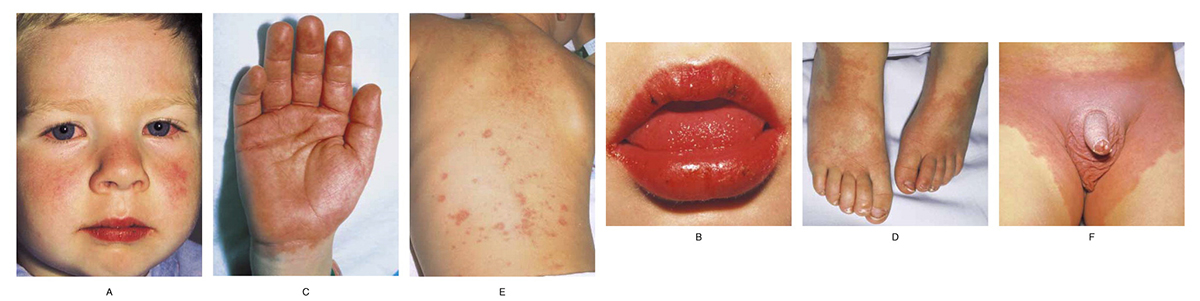
- “Pink eye” (conjunctivitis) without a discharge (Photo A)
- Rash on the body (trunk) and genital area (E & F)
- Extremely red, swollen tongue (strawberry tongue) with red, dry, cracked lips (B)
- Red, swollen rash on the palms of the hands and the soles of the feet (C & D)
- Swollen neck lymph nodes and perhaps elsewhere
- Irritability
Phase Two
- Peeling on the hands and feet, especially the tips of the fingers and toes, often in large sheets (Photo above)
- Joint pain
- Diarrhea
- Vomiting
- Abdominal pain
Phase Three
- signs and symptoms slowly go away unless complications develop
- It may be as long as eight weeks before energy levels seem normal again
Symptoms Doctor’s Key In On
- Any higher than average fever (101.6 F) lasting > 5 days – especially with mouth sores.
- Any brilliantly red lips, tongue rash – especially with “pink eye.”
- Any rash on palms or soles – especially with peeling.
There are so few diseases which cause these three symptoms that Kawasaki’s Syndrome must be “ruled out” whenever they are seen – and peeling of fingertips is almost a sure sign.
Treatment
Current thought is that certain genes predispose toward Kawasaki Syndrome in which an unknown “environmental trigger” causes the body to “self-inflame” its medium-sized arteries.
Except for a few rare individuals, hospital treatment with immune serum and aspirin enables most children to recover without serious problems. Treating within 10 days is enough to greatly reduce the chances of lasting damage; which, because they are in the heart and vessels, are often serious.
– – 0 – –
We’re almost half way through the updated list of childhood diseases parents should know about. We’ll talk again in part five where we’ll begin with… Chicken Pox.
11 Posts in Childhood Diseases (childdiseases) Series
- Part 10 - Lyme - Allergies – 9 Oct 2014
- Part 9 - Impetigo - Influenza – 1 Oct 2014
- Part 8 - Polio - MRSA – 23 Sep 2014
- Part 7 - Meningitis - Scarlet Fever – 11 Sep 2014
- Part 6 - Diptheria - Tetanus – 3 Sep 2014
- Part 5 - Varicella - Rubella – 18 Aug 2014
- Part 4 - Rotavirus - Kawasaki's – 10 Aug 2014
- Part 3 - Hand, Foot, Mouth and Fifth disease – 29 Jul 2014
- Part 2 - Otitis, Glue ear – 21 Jul 2014
- Part 1 - Croup, Bronchiolitis – 17 Jul 2014
- Childhood Diseases Parents Should Know: Intro/Index – 15 Jul 2014
Advertisement by Google
(sorry, only few pages have ads)