
Medical Marijuana

Perhaps most, if not all, of you think of gangsters, terrorists, drug dealers and low-life “users” when you think of the word marijuana. And, with all the idiocy going on by politicians over “legalization” you might also think of societal breakdown, corruption, destruction of families… loss of moral values.
Or, after being beaten into a frazzle by the constant bombardment of so-called “do-gooders” on the media, you may be starting to feel guilty for living the life you’ve always lived trying to do right, knowing what you know about human nature and thinking what you think about the good and evil you’ve seen all around you during your life.
Marijuana and tobacco while pregnant—one and the same. The commitment of a child to life-long medical, emotional and intellectual issues.
Well, you should to the first and shouldn’t to the second. Marijuana IS STILL (and perhaps even more so) the leading “gateway drug” to a life of crime and decadency for the youth of every country.
And there are still HUGELY EVIL ulterior motives in every political decision made. If we had access to the real truth I’m sure we would find many straight pipeline-links from our decision and policy makers directly to organized evil.
Looking Beyond The Smoke
Marijuana: Medical Uses
As absurd as it sounds however, marijuana is a pharmaceutical in the same sense that nearly every other narcotic and soporific is and there were just bound to be a few unique uses for it in medicine—which people have now found.
Let’s see what we know about the very, very limited medically legitimate uses for marijuana
Reality and Terms
Make no doubt, Marijuana is still the most widely cultivated, trafficked and abused illicit drug. The word Marijuana, or cannabis, refers to the dried leaves, flowers, stems and seeds of a particular genus of hemp plant—C sativa. “Hashish” or “Hash” is the unpollinated female plants concentrated in a resin. “Hashish oil” or “cannabis oil” uses solvent to extract the psychoactive resin from the plant and concentrate it.
Five-thousand years ago the Chinese (along with their opium dens) discovered and used cannabis to alieve pain and cramps—in addition to its other brain activities. It was used in ancient Greece, Rome, Middle East and North Africa as well.
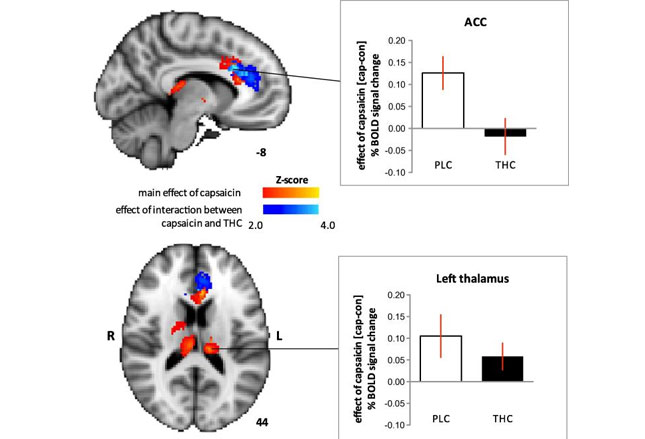
Scientists today have the machines to actually “watch” the brain when they give people hot peppers (capsaicin – red in the graphic) and THC (cannabis – blue in the graphic).
My including the graphic is only to show you that we can actually see where THC works, where it doesn’t and that it’s not just a placebo effect (PLC in the graphic).
History and Politics
Introduction and use of marijuana in 1910 by Mexican immigrants following their revolution caused US popular disgust over the social and economic ills it immediately caused in this country. US Congress first taxed marijuana then criminalized it to discourage then prohibit use.
The “war on drugs” (1970-71) increased federal activity and harshened sentencing till it became “schedule I” (no accepted medical use, high abuse potential). California legalized limited “compassionate use” under physician prescription in 1996.
A few other states followed suit; then, in 2016 enough elected officials with marijuana “sympathies” had hold of the political system in Colorado to further liberalize its use in that state. Again, a few others followed suit making them inconsistent with federal law AND international law.
In 2015, the “feds” (US) took their lead from what the motion picture industry did after the public furor over the release of “gremlins” and created a “r” rating. By making marijuana and its derivatives the new “schedule 1-r” makes medical research on the stuff a bit easier.
Despite the tiny number of countries legalizing marijuana, international law still prohibits cannabis resin smoking and the non-medical use of cannabis. In 2013 and 2016 the UN officially warned Obama that US policies were inconsistent with international law.
The plant is still heavily used in Mexico and its supreme court has ruled in favor of “recreational use.” Portugal “decriminalized” ALL drugs in 2001 making them “administrative violations.” In their tiny, very specific culture they claim (so far) to have “no severe consequences” but can’t report comprehensive verifiable data to the assertion.
Make no mistake. The vast majority of the motivation behind marijuana legalization has been due to “vested interests” (both political and entrepreneurial) and not a lick because of legitimate clinical reasons.
I’ll assert again that the legitimate medical research system would have already had all the beneficial medical uses and dangers sorted out years, perhaps decades, ago if politicians hadn’t intervened with their vested interests.
The Body’s “Cannabinoid System”
It’s obvious that the human body has some internal hormone or chemical somewhere which acts on some receptor resembling that of marijuana’s THC—otherwise the plant would only be useful for making rope and we would not be having this discussion. Well, recent research has “discovered” that system and, for want of a wiser and better term, it’s called the “endocannabinoid system” (ECS).
And you already know what it does just by knowing what marijuana does—regulatory functions in the heart, digestive, endocrine, immune, nervous and reproductive systems (i.e. pleasure, memory, thinking, concentration, movement, coordination, sensory and time perception, appetite and pain).
And we even know that there are two types of those receptors in the body: type 1 (in the nervous system) and type 2 (in the peripheral organs)—just like all the other regulatory systems and receptors in the body we already know about. When allowed by all the needless and difficult political regulations, this is where research is trying to make some headway.
Research
It seems that nearly every researcher has a “favorite” disease they want to try cannabis on. Most of the time there is a big fat zero for results; but, on a very, very… very rare occasion, there is some kind of effect. Although much, much… much less frequent than what the entrepreneurial growers and “pushers” try hard to get you to believe.
What legitimate science is trying to focus on now is the same thing we’ve been focusing on for years: obtaining something useful WITHOUT unwanted or dangerous side-effects.
Plain THC stimulates appetite, reduces nausea and MIGHT reduce pain, inflammation and/or spasticity; whereas, its isomer CBD [cannabidiol] does all that PLUS it is NON-psychoactive (doesn’t get you high) and might additionally control seizures, treat psychosis and addictions.
In 2015 an extensive review of all legitimate research to that date was performed and found that only a limited number of them were legitimate research studies. After culling the clearly worthless experiments, they were left with 97 trials having 6,492 participants.
Had they all been legitimate, unbiased studies those numbers could have meant something; but, depressingly, only 4 of the 97 (5%) were judged to have a “low risk” of bias. All the rest (93) had high or unclear risk of having biased results!
Moderate-quality evidence for therapeutic use was deemed possible only for: chronic pain and spasticity. There was only low-quality evidence for a “suggestion” of its use against: Nausea/vomiting in chemotherapy, appetite stimulation in HIV/AIDS, sleep disorders and tic severity in Tourette’s.
What they did find evidence of, but you never saw played out in the press, was a higher than previously thought risk for short-term adverse events (psychiatric, nervous system, musculoskeletal and blood disorders).
Needless to say, legitimate researchers are now desperately trying to distinguish fact from fiction with unbiased studies; but, politicians have actually “blocked” research with their bizarre rules against research while at the same time trying to cater “empathy-votes” by appearing to be “caring” about “medical conditions.”
If our “so-called” elected officials would just get out of the way of legitimate research we would have already had this legitimately sorted out years ago!
Clinical Considerations of Medical Marijuana

Currently there are five clinical categories where medical marijuana is being tested: pain, nausea and vomiting (i.e. cancer), weight loss in debilitating disease, neurologically induced spasticity and “other.”
The US government has “authorized” three strengths for research: “low, medium and high—1.3, 3.5 and 7% THC respectively.” UNFORTUNATELY, the only strengths available in pharmacies to actual patients are all greater than 10% and up to 30% of THC!!!
So, thanks to the politicos who don’t have a clue what they are doing, US scientists can’t even do research on the very drugs available to patients!!!
In addition, the yahoo’s have “fast-tracked” cannabinoids in diseases with low-quality evidence and left patients having multiple sclerosis with the choice to move out of the country in order to obtain drugs available in TWENTY-SEVEN other countries!
Verifiability and Safety
In case you’re thinking that the government, who is liberalizing marijuana use, is concomitantly taking steps to see that either the users or public is safe—think again.
It’s the legitimate researchers WHO ARE JUST NOW publishing “suggestions” for things a physician should “think about” before “plopping a patient over the fence into the marijuana patch.”
Things such as: verifying the diagnosis, checking that actual “signs” and physical examination verify the diagnosis, verified trial of standard therapy and treatment response and degree of risk for drug abuse addiction and/or diversion. You know, the simple procedure we all follow for EVERY OTHER DISEASE WE TREAT!

Currently there is no evidence demanded that any physician has discussed even the rudimentary precautions inherent in an addictive drug, i.e.:
• Diversion/inappropriate use
• The risks of marijuana use, particularly in vulnerable populations
• Methods of administration (oral vs vaporization [preferred] vs smoking)
• Periodic evaluation of therapeutic efficacy and appropriateness
• Not operating machinery or a vehicle during cannabis use
• Withdrawal/cessation strategies, such as tapering/slowing
In addition, patients should be informed that medical authorization is not protection against job loss, and physicians have the right to discontinue cannabis treatment.
Routes of Administration
This topic is not a joke. The methods chosen by drug abusers for years (ingestion and smoking) are the most dangerous and damaging ways to receive the legitimate benefits of THC.
Ingestion (think brownies) is dangerously variable in amount and timing of absorption (especially for the pediatric and adolescent population). It can vary from ZERO to massive amounts in one to SIX hours after swallowing.
There is absolutely NO use for such a hit-and-miss method of dosing in legitimate medical care and has not only produced increased ED visits but also deaths.
Druggies used smoking most often and it still remains the most common route of administration despite the large quantity of evidence regarding its adverse pulmonary effects!
Although vaporization is not without risk, the side effects appear to be less than those from smoking cannabis; thus, it is probably the best route of administration at this time.
☤
The best thing that could happen for societies best good would be for lawmakers to get their hands out of medical marijuana research! What they’ve done has gotten us into an intolerable mess; which, unfortunately, now may only be remedied by national public referendum or recall/impeachment. Medical research will make sense of this, IF given the chance.
Next in this unintentionally long series: What, if anything, marijuana is good for?
5 Posts in Marijuana (marijuana) Series
- What It's Good For – 12 Oct 2017
- Medical Marijuana – 4 Oct 2017
- Medical marijuana, test what you know – 25 Sep 2017
- Prenatal Marijuana & Brains – 21 Sep 2017
- Marijuana Series: Intro/Index – 20 Sep 2017