
Parenting: Circumcision
Infant Circumcision
Trying to clear the hysteria!
by Gregory A. Barrett, M.D.
The fate of the foreskin has a curious place in the lore of American medicine. Around the turn of the previous century physicians here began to hold the opinion that there were measurable medical benefits to circumcision including basic hygiene, prevention of venereal diseases, and the avoidance of cervical cancer in females who were so unwise as to mate with a man who had an intact foreskin. Parents were thus informed of these beliefs with, one may presume, considerable gravity. They may have even been given an onerous set of instructions regarding the care of the uncircumcised penis, should they opt to go against medical advice.
Actually, the care of the uncircumcised foreskin is roughly the same as that of the right thumb—simply clean the outside and otherwise leave it alone. That’s basically all there is to it; the adhesions will break naturally on their own with time.
Circumcision: current practice
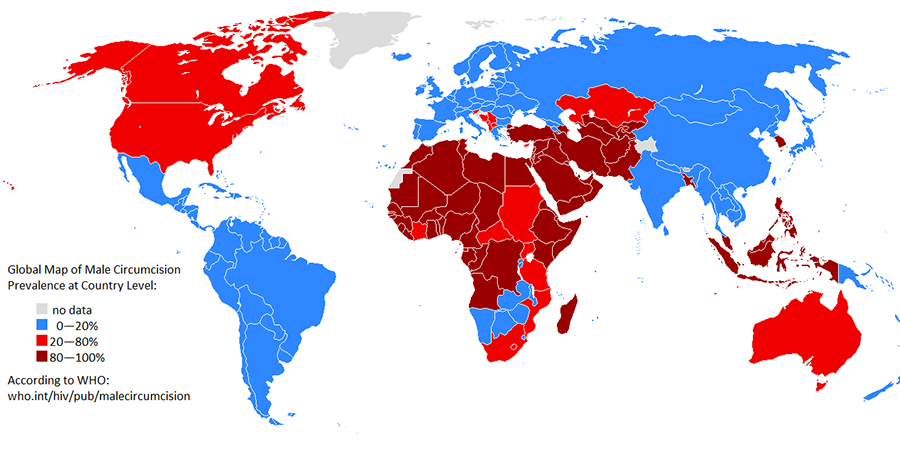
The rest of civilization outside our borders, the British in particular, never really bought into the belief that circumcision was medically necessary. Nonetheless the practice took hold on this side of the Atlantic and thus three to four generations of American males were circumcised.
In the seventies and eighties, a “fresh” look was taken at these beliefs in light of developing vocal protests over the procedure. Supposedly applying appropriate control groups and modern scientific methods, “new” studies arrived at different conclusions. Previous rationalizations for the procedure then seemed incorrect. As it turned out, circumcision didn’t prevent all urinary infections, gynecological cancer seemed to have nothing to do with the circumcision status of the woman’s partner, and the likelihood of a male acquiring a venereal disease is far more dependent upon the sexual history of his lady friend than the length of his foreskin.
Benefits

There do exist a few benefits: circumcision is relatively protective against both uncomplicated bladder infections in the first year of life and cancer of the penis, a very rare disease usually limited to elderly men. Furthermore, should a male choose to practice unprotected sex, recent studies indicate his risk of acquiring a venereal disease may indeed be somewhat higher if he still has an intact foreskin, although abstinence, good judgment, and proper application of a condom remain far more beneficial.
Risk/benefit analysis of these factors (the holy grail of determining the validity of a medical intervention) led the American Academy of Pediatrics to state that: there didn’t seem to be any medical evidence supporting the practice; although there didn’t seem to be such a risk in the procedure that would warrant advising against it. That advice held for several years.
Since there may no longer be a valid reason for circumcision one would have assumed the custom would have quietly disappeared. Why would parents subject their newborn son to a surgery if there is no measurable medical benefit? The simple truth is that old habits are slow to die. Within the U.S. there seems to be significant geographic differences—the west coast performing the least, the southern states the most.
Why?

There are several other reasons that parents continue to sign the consent form. First of all is religion of course, the Jewish faith most predominantly in America, along with a host of others. Additionally, and related, for many families A key factor is whether or not the father is circumcised. It seems critical to have the sons resemble their fathers in this important aspect.
Another major issue is what I refer to as: “The Eighth Grade Locker Room Argument.” The key concern here is the makeup of their son’s future gym class fourteen years hence. And the answer to that query is that the overwhelming majority of his peers WILL be circumcised.
Generally, the father is allotted fifty-one percent of the vote on this subject, his spouse acquiescing quietly to his superior judgment. (For many of us this will be the one and only occasion we ever get majority say about ANYTHING involving our children, although none of us realize it at the time….)
Risks
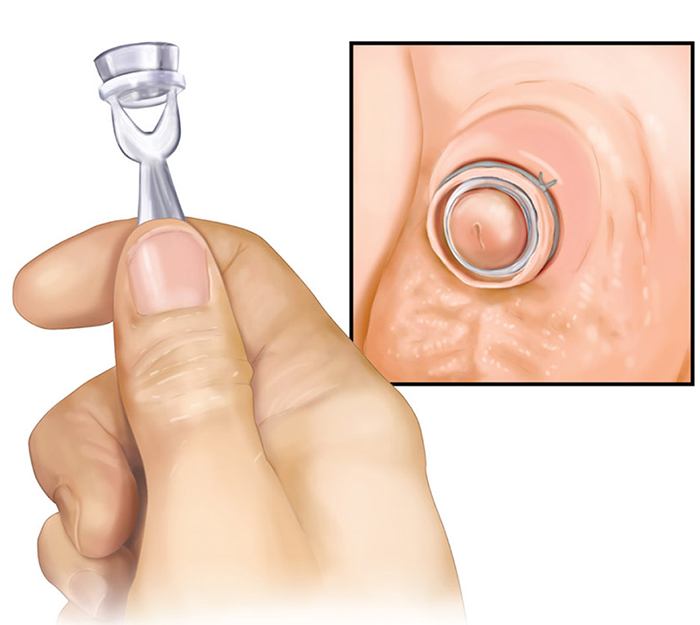 >
>A circumcision is actually not nearly as dangerous and brutal as many would have one believe. The risks of the procedure are those universal with any surgery and in practice are remarkably rare. Trimming a hangnail probably carries roughly the same potential of bleeding and infection as a circumcision. Pain can be an issue, but physicians have become much more sophisticated and skilled regarding this in recent years.
It wasn’t very long ago that the baby boy was simply strapped on a papoose board and circumcised without any anesthesia.
Nowadays by injecting lidocaine (without epinephrine) underneath the skin at the base of the penis for a digital block, in combination with the sedative effect achieved by having the infant suck on a sugar-containing substance (sucrose), the procedure is relatively benign. Some babies really do immediately go into a zone, once they get that first taste of the sucrose, making one speculate as to whether this could be a possible future predictor of a sweet tooth. Time will tell….
What did I do myself?
In case you’re wondering about what we did with our own son; well, that is a bit of a funny story. During the latter stages of my wife’s second pregnancy, she spent much of her time haggling with me over: 1- the choosing of a boy’s name (I, holding out for monosyllabic, masculine-appropriate; and her list of acceptables seemingly inspired by the names of baby dragons in fantasy novels); and 2- the reading of anti-circumcision literature.

Armed with information gleaned from “The Rape of the Foreskin” pamphlet and the like, she asked me at dinner one night if I had strong feelings about circumcision. I assured her I did not, honestly feeling the whole topic is much ado about nothing. She said she just didn’t see any legitimate justification in favor of having it done and unless I had a significant argument to the contrary, she would prefer we pass on the option. I told her no problem and she smiled with relief, gave me a hug, and expressed her gratitude at my open-mindedness.
Sensing an opportunity I decided to press my luck. “John?” I suggested.
“No!” she replied in horror.
“Arganon?”
“Forget it.”
A couple of weeks later, more or less right on schedule, our baby boy arrived. On the second hospital day the two of us were sitting in our hospital room with Keith and a familiar smell wafted up from the bassinet. My wife volunteered to do the change and paused midway, staring down in confusion at the newest addition to our family.
“Is there a problem?” I inquired.
“Well,” she said hesitantly, “I don’t know.”
“What is it?”
“I’m not sure.”
I rose from my chair and strolled over to join her. “Yes, dear?”
“I was just wondering…what is that?”
“What is what?”
“That,” she said, waving her hand vaguely in the general direction of our son’s genitalia.

“That?”
“Yeah. That…”
“That,” I pronounced in my most authoritative pediatric intern voice, “is an uncircumcised male penis.” (At least I knew something.)
“Hmm,” she said thoughtfully.
“What is it, dear?”
“Well,” she replied, shaking her head slowly as she arrived at a decision, “that’s simply not going to do.”
The following morning my son was circumcised. And thus, I have added, “What is that?” to my list of reasons for parents having their newborn boy circumcised.
What to do?
So, in the final analysis, what should one do? Even today, centuries later, it remains a valid question. In the end it’s not all that critical clinically; because, whatever is decided, the odds are overwhelming everything is going to turn out just fine. There will be much more critical decisions to make as a parent later on down the line… believe me.
☤

Gregory A. Barrett, M.D. graduated in 1978 from the Ohio State University College of Medicine and went on to subspecialize in Pediatrics at Columbus Children’s Hospital. He set up practice in Columbus Ohio where he met and married is wife Darla and raised two children Rachel and Keith. He authored a respected blog “Real Pediatrics” which he dedicated to his wife after she passed from cancer in 2008.
[Dr. Barrett’s last post was in 2021 and his blog is now abandoned. There is a company camped on it and asking an exorbitant amount of money for the URL “Real Pediatrics,” I’m sure massively more than the good doctor ever made from his “labor of love.” I can’t stand the idea that all his good work will evaporate into thin air; so, until advised otherwise, I’ve determined to keep his stories and advice alive on this blog. Perhaps we will both meet one day and compare stories.]
Advertisement by Google
(sorry, only few pages have ads)