
State of Immunizations: 2017
Believe it or not the brand spankin’ new immunization schedule just released has actually LOWERED the number of immunizations recommended for teens!
I know, it’s hard for me to comprehend too; but, we’ll take it while it lasts.
Teen amazed at new immunization schedule with one less shot
It’s a never ending effort to keep up to date these days with all the new information we’re getting about immunology. In the days of Jenner and Salk it was comparatively simple to create and market their immunizations.
The likely alternative was death, and it occurred in nearly every family so everybody knew bout it. And the procedures either worked or they didn’t and if they did everyone soon found out about it and wanted it for their children. Once they were accepted little else was thought about them—comparitively speaking that is.
Today, not so much. We want to know the best dose, the best timing, the side-effects to the nth degree, a cheaper way to make them… and on and on ad-infinitum.
Literally thousands of research studies are done each year. So many that I certainly can’t read them all—or even know about them. BUT, I’m sure glad there are some people who do, working at the CDC and the AAP.
Immunization Schedule For Children and Teens
Highlights of changes for 2017
There are four major changes in this years recommendations resulting from new research this year. In addition there are several smaller “tweaks” in timings and indications.
HPV Vaccine
Teens will be pleased to know that they’ve found out that receiving three doses of HPV vaccine doesn’t protect any greater than receiving two doses.
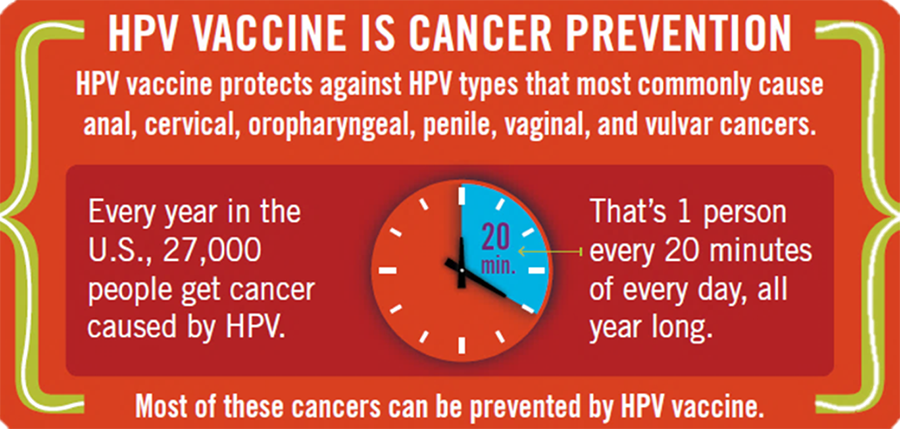
So, the previous recommendation to receive three doses beginning at age 11 or 12 has actually been reduced to TWO doses of HPV vaccine and now they can be given anywhere between 9 and 15 years of age.
The catch is though, if you don’t get your first dose on or before your 15th birthday, you need to go back to the three doses in order to obtain protection against the cancer.
This immunization does sting a bit more than other shots and has unfortunately gotten caught up in a huge amount of misinformation and hysteria on the internet. The earlier the immunization is received the better its protection for the child who receives it. It DOES actually protect both girls and boys from various types of cancers attacking both genders.
Additionally, the timing has been modified. Although the HPV series was initially begun “early” for those children who were “at risk,” researchers have found that it can be given at 9 to 10 years of age for all children.
Hepatitis B
Prior to this year the practice has been to give one dose of the monovalent Hepatitis B vaccine “at birth.” Which to some has been taken to mean “within 2 weeks of birth.”
That has been found to be less effective, especially for the 25,000 infants whose mothers happen to be chronically infected with hepatitis B.
The rate of transmission from infected mother to newborn infant is 90% so waiting until the first office visit is unacceptable. If babies are infected at birth, they not insignificantly develop cirrhosis or cancer of the liver.
Now, the guideline has been changed to read: First of three Hepatitis B vaccine doses for “all newborn children within 24 hours of birth.”
Sometimes doctors caring for the newborns assume the mother is negative so the vaccine can wait until the first office visit; which, in the US, has missed about 1000 babies every year. Now, pediatricians should see that the baby goes home after having the first dose.
Live Attenuated Influenza Vaccine

We were already told earlier in the year that the live attenuated influenza vaccine, often given to children because it can be given orally, has been shown NOT to WORK effectively against influenza.
We were advised against giving it to anyone but now it has been taken completely out of the recommendations and is no longer an option for children.
It’s still being made and is available but the experts say “it hasn’t worked at all” in the last three influenza seasons. The oral influenza vaccine should not be given to children under any circumstances for this 2016-2017 influenza season.
Tdap
The “Tdap” vaccine is the new formulation against Tetanus, Diphtheria and Pertussis (Whooping Cough), extremely deadly diseases which have largely been eliminated in developed countries. Except of course, the isolated areas of un-vaccinated people due often to preferential reasons.
In those areas, infants still die of whooping cough; because, like I said, the disease has been “eliminated” NOT “eradicated.” The bacteria is still around in the population awaiting spread to an unvaccinated newborn.
The “Td” is a “booster” dose against Tetanus and Diphtheria. Adults should receive one every 10 years. “Tdap,” on the other hand, not only protects against Tetanus and Diphtheria but also Pertussis too. A single lifetime dose of Tdap is recommended for everyone—except pregnant women who get it more often.
The problem with immunizing against Pertussis is that the people who suffer the most severely, and die the most often, are newborns and infants under 2 months of age. That is also the time BEFORE they are able to develop antibodies from receiving their own immunizations!

Therefore, we immunize mothers with a Tdap dose every time they become pregnant.
What they’ve found out now is that the earlier in the gestation a pregnant woman recieves the booster shot, the higher the concentration of protection given to the baby at birth.
Now, the guidelines for immunizations have been changed to read: “vaccinate mothers (with Tdap), including adolescent mothers, as early as possible in the 27- to 36-week gestational window.” When the immunization is given closer to 27 weeks the baby is born with higher concentrations of maternal antibodies against Whooping Cough.
Other changes (Tweaks) to timing and wording
The recommendations for “catch up” immunizations have NOT changed in this years schedule. However, there were a few other “tweaks” made to the wording for some vaccinations and the display graphics; largely to make things more clear and understandable.
- A column was added for 16 year old adolescents to be separate from 17-18-year-olds and emphasize their need for a quadrivalent meningococcal conjugate vaccine (MenACWY) booster.
- Meningococcal ACWY is now recommended for children with HIV.
- A new table addresses which vaccines may be indicated for children and adolescents who have specific conditions; namely, kidney, heart, liver disease or diabetes, or who have a cochlear implant.
The CDC has updated their “official” web page with the latest recommendations and can be found in full here.
[Pediatrics. Published online February 6, 2017]